Download
1 / 12
120 likes | 334 Vues
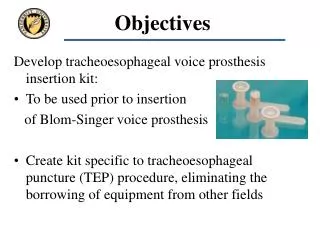
Objectives. Develop tracheoesophageal voice prosthesis insertion kit: To be used prior to insertion of Blom-Singer voice prosthesis Create kit specific to tracheoesophageal puncture (TEP) procedure, eliminating the borrowing of equipment from other fields. Relevance.

E N D
Objectives Develop tracheoesophageal voice prosthesis insertion kit: • To be used prior to insertion of Blom-Singer voice prosthesis • Create kit specific to tracheoesophageal puncture (TEP) procedure, eliminating the borrowing of equipment from other fields
Relevance • There are about 50,000 post-laryngectomy patients living in the U.S. • 12,500 new cases of laryngeal cancer are diagnosed each year with approximately 9,000 of these patients surviving treatments, including surgery, chemotherapy and radiation. • We estimate 2,000 - 3,000 patients could benefit from our product each year.
Safety Issues Considered • Diameter of Esophagus: To avoid unintended damage to the esophagus, both opposite puncture and distally toward stomach, our design included an angled tip. • Ease of Use: Angled tip for location in scope and grabbing by forceps and overall length to allow for handling. • Diameter of Trachea: This was considered in order to allow sufficient manipulation by physician. • Materials: Chosen to be non-reactive with human body. • Designsafe: Completed analysis for consideration of human error.
Designs Considered • Catheter with sharp, biodegradable tip designed for puncture and distal insertion into esophagus in one step. This would eliminate the need to pull the catheter up the esphagoscope and then force it back down the esophagus. The biggest problem with this design came in finding a material that would be strong enough to puncture esophagus and at the same time would dissolve quickly enough to prevent internal damage to esophagus. • Catheter receptor that can be forced through the esophagus and pulled out of the mouth through the esophagoscope. After it is pulled out of the scope the catheter is to be detached and sent back distally towards the stomach in the esophagus where it remains for 5-7 days. We considered various means of attachment for the catheter including hooks, clamps, and screw-like threads.
Design Chosen • Hook extends into device cavity 2mm • Standard red rubber catheter included in package • Prototypes are made out of stainless steel, actual product will be made of plastic (possibly PVC)
Materials • For our prototype we chose to use 304 stainless steel because we could create a sample device in the machine shop. We specifically chose stainless steel because it does not react with the body, does not corrode quickly, and can be heated to temperatures high enough for sterilization to take place. The disadvantages of using steel as a disposable material lies in the cost of the metal when compared to a plastic. If this stainless steel was the final material chosen, our product would not be disposable and doctors choosing to use it would save the tip for cleaning and sterilization between procedures. • We recommend the use of our design to create a mold for use with plastics. We believe that PVC (Poly-vinyl chloride) is an ideal biomaterial because it is cheap, tough, non-reactive, and easily machined. It can also be made translucent to allow for easier attachment of the red rubber catheter. These properties are ideal for a the disposable kit that we want to create. One flaw that exists with PVC is that it is not biodegradable and must be incinerated at high temperatures that cause it to release toxic fumes into the environment.
Calculations We chose the angle q to allow for a sufficient sharpness at the tip of our device. We looked at various angles and decided that a tip angle of 12º is sufficient. We used the value of 3/8” for the value d because that is the diameter of the steel rod we used. Based on this the length L came out of the above equation: 1.78”. This actual length is shorter on the device because of our angled tip. We were able to choose the value for x (0.4” in our sample) to allow the surgeon to hold onto the device and maneuver it through the esophagus and into the esophagoscope.
How is our device used? Puncture hole made with our device Forceps used to pull device through esophagoscope Device removed and catheter forced back down esophagus
Recommendations • The examination of the prototype by Dr. Day and other physicians for the purpose of testing the design and realizing alterations for the final design. • Create another prototype including changes recommended by Dr. Day as well as those that we see as beneficial. The latter include lengthening the device for easier use, the shrinking of the angle at the tip to allow for easier grabbing with the forceps, and the widening of the hole at the back of the device. • Locate a company willing to manufacture device and complete kit (device with red rubber catheter included) for use by surgeons. • Consider patenting or licensing of design.
References • Blom, Eric D., Hamaker, Ronald C., “Tracheoesophageal Voice Restoration Following Total Laryngectomy,” Cancer of the Head and Neck , W.B. Saunders Publishers 1996, pgs. 839-851. • Hamaker, Ronald C., Hamaker, Ronda A., “Surgical Treatment of Laryngeal Cancer,” Seminars in Speech and Language, Volume 16, Number 3 August 1995, pgs. 221-231. • Economou, Steven G., Atlas of Surgical Techniques, W.B. Saunders Publishing, Philedelphia 1996, pgs. 82-98. • Hill, David, Design Engineering of Biomaterials for Medical Devices, John Wiley & Sons Ltd, 1998. • Kao WW., Mohr RM., Kimmel CA., Getch C., Silverman C., “The Outcome and Techniques of Primary and Secondary Tracheoesophageal Puncture,” Archives of Otolaryngology and Head and Neck Surgery 1994 Mar: 120(3):301-7. • Leder, Steven B., Erskine, M. Cara, “Voice Restoration After Laryngectomy: Experience with the Blom-Singer Extended-Wear Indwelling Tracheoesophageal Voice Prosthesis,” Head and Neck, September 1997, pgs. 487-493. • Myers, Eugene N., Operative Otolaryngology Head and Neck Surgery Volume I, Saunders, W.B. 1997, pgs. 444-455. • Quer, Miquel, Burgues-Vila, Joaquim, Garcia-Crespillo, Pedro, “Primary Tracheoesophageal Puncture vs Esophageal Speech,” Archives of Otolaryngology and Head and Neck Surgery, Volume 118, February 1992, ppgs. 188-190. • Ratner, Buddy D., Biomaterials Science: An Introduction to Materials in Medicine, Academic Press 1996, pgs. 57-60. • www.inhealth.com
Tracheoesophageal Voice Joshua Fox and Sponsor: Terry A. Day, M.D. Vanderbilt University
Prosthesis Insertion Kit Michael Hixson (Department of Otolaryngology) Biomedical Engineering