Download
1 / 47
470 likes | 721 Vues
Not tonight Honey, I have a headache…. The trials and tribulations of Female Sexual Dysfunction. Kim O’Connor, MD University of Washington General Internal Medicine. Outline. Sexual Response Cycle Categories of Female Sexual Dysfunction Appreciate the biopsychosocial influences History

E N D
Not tonight Honey, I have a headache….The trials and tribulations of Female Sexual Dysfunction Kim O’Connor, MD University of Washington General Internal Medicine
Outline • Sexual Response Cycle • Categories of Female Sexual Dysfunction • Appreciate the biopsychosocial influences • History • Evaluation • Treatment
Clinic Visit: Mrs. Jones HPI • 34 year old female • 6 months post partum, vaginal delivery, breast feeding • She comes in to speak with you about some sexual health concerns. • She states that “sex just isn’t like it used to be and I am worried that something is wrong with me.” PMHx • Hx of anxiety and depression since childhood • Seasonal allergies • Insomnia Medications • Norethindrone 0.35 mg po qd (Micronor) “Minipill” • Citalopram (Celexa) 20 mg po qd • Diphenhydramine (Benadryl) 25 mg po qhs
The biopsychosocial factors impacting sexual function Family Beliefs Mental Health Medical History Early Sexual Experiences Sexual Function Illness/ Medications Partner Relationship Cognitions/ Beliefs External Stressors Partner’s Sexual Functioning
Screening For FSD • Physicians do not regularly screen for FSD -Only 10-20% of women will spontaneously volunteer info about FSD to their doctor • Screening questions • “Sexuality is such an important part of our overall health and I’d like to ask you some questions about that now. Is that okay with you?” • “Do you have any concerns about your sexual health?” • Female Sexual Function Index
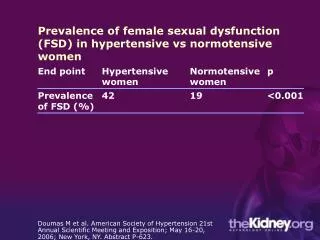
Female Sexual Dysfunction • Sexual complaints occur in 40% of women • Only about 12% are associated with distress • Symptoms MUST: • Be recurrent or persistent • Cause significant personal distress or interfere with personal relationships • Primary (lifelong) vs. Secondary (acquired) • Situational vs. generalized
Classifications of FSD* • Desire • Hypoactive sexual desire disorder - MOST COMMON • Sexual aversion disorder • Arousal • Decreased arousal • Orgasm • Difficulty achieving orgasm, anorgasmia • Pain • Dyspareunia, vaginismus, non-coital pain • Disorder due to general medical condition • Disorder due to substance abuse or medication *Based on traditional linear model of female sexual response cycle
Clinic Visit: Mrs. Jones Additional history from Mrs. Jones... • 6 months post partum, vaginal delivery, breast feeding • Husband upset because they aren’t having sex very often. She also wishes she were more interested in sex. PMHx • Hx of anxiety and depression since childhood • Seasonal allergies • Insomnia Medications • Norethindrone 0.35 mg po qd (Micronor) “Minipill” • Citalopram (Celexa) 20 mg po qd • Diphenhydramine (Benadryl) 25 mg po qhs
Desire Disorders • Feelings of desire may not occur prior to the onset of sexual activity • No sensation of desire during ANY part of the sexual cycle
Desire Disorders • What questions do you want to ask our patient?
Desire Disorders • “Are you having any problems with desire or interest in sex?”
Desire Disorders • “Are you having any problems with desire or interest in sex?” Yes, tired all the time. New baby. Feeling fat.
Desire Disorders • “Are you having any problems with desire or interest in sex?” • “Are you bothered by your decreased level of desire or interest?”
Desire Disorders • “Are you having any problems with desire or interest in sex?” • “Are you bothered by your decreased level of desire or interest?” Yes, both because my husband is upset and I wish I wanted to be more sexually active.
Desire Disorders • “Are you having any problems with desire or interest in sex?” • “Are you bothered by your decreased level of desire or interest?” • “In the past was your level of sexual desire or interest good or satisfying to you?
Desire Disorders • “Are you having any problems with desire or interest in sex?” • “Are you bothered by your decreased level of desire or interest?” • “In the past was your level of sexual desire or interest good or satisfying to you? Actually, it was fantastic!
Desire Disorders • “Are you having any problems with desire or interest in sex?” • “Are you bothered by your decreased level of desire or interest?” • “In the past was your level of sexual desire or interest good or satisfying to you? • “Is sexual activity pleasurable for you or does it cause you severe distress or anxiety?”
Desire Disorders • “Are you having any problems with desire or interest in sex?” • “Are you bothered by your decreased level of desire or interest?” • “In the past was your level of sexual desire or interest good or satisfying to you? • “Is sexual activity pleasurable for you or does it cause you severe distress or anxiety?” Pleasurable.
Desire Disorders • “Are you having any problems with desire or interest in sex?” • “Are you bothered by your decreased level of desire or interest?” • “In the past was your level of sexual desire or interest good or satisfying to you? • “Is sexual activity pleasurable for you or does it cause you severe distress or anxiety?” • “What factors do you think may be contributing to your decreased interest or desire?”
Desire Disorders • “Are you having any problems with desire or interest in sex?” • “Are you bothered by your decreased level of desire or interest?” • “In the past was your level of sexual desire or interest good or satisfying to you? • “Is sexual activity pleasurable for you or does it cause you severe distress or anxiety?” • “What factors do you think may be contributing to your decreased interest or desire?” The new baby, feeling depressed, breast feeding, no help from my husband…
You are concerned that she has Hypoactive Sexual Desire Disorder (HSDD) Which ONE or SEVERAL of the following MAY be contributing to her HSDD? • Depression • Norethindrone (Micronor) “mini-pill” • Stress • Breast feeding • Hypothyroidism
Desire Disorders * Items in red are present in our patient
Clinic Visit: Mrs. Jones Additional history from Mrs. Jones… • She reports that even if she wants to have sex her body just doesn’t seem to respond. • She also complains of poor lubrication. Medications • Norethindrone 0.35 mg po qd (Micronor) “Minipill” • Citalopram (Celexa) 20 mg po qd • Diphenhydramine (Bendaryl) 25 mg po qhs
Arousal Disorder • Persistent or recurrent inability to attain or maintain sufficient sexual arousal • May be subjective, objective or both • MUST occur in the setting of ADEQUATE stimulation
Which of her medications is MOST likely contributing to her arousal disorder? A. Norethindrone (Micronor) “mini-pill” • Citalopram (Celexa) • Diphenhydramine (Benadryl)
Arousal Disorders * Items in red are present in our patient
Clinic Visit: Mrs. Jones Additional history from Mrs. Jones… • She is frustrated because she is having a difficult time having orgasms • This was rarely a problem for her in the past • She wonders if the vaginal delivery damaged any of the nerves “down there” Medications • Norethindrone 0.35 mg po qd (Micronor) “Minipill” • Citalopram (Celexa) 20 mg po qd • Diphenhydramine (Benadryl) 25 mg po qhs
Orgasm Disorders • Lack of orgasm, markedly diminished intensity or delay of orgasm DESPITE self-reports of high sexual arousal or excitement. • Primary vs. Secondary Disorder • Has the patient ever achieved orgasm with their partner or via self-stimulation?
Which of the following conditions is UNLIKELY to contribute to an orgasm disorder? • Type 2 Diabetes Mellitus • Vaginal delivery • Hypertension • Spinal cord injury • Multiple Sclerosis
Orgasm Disorders * Items in red are present in our patient
Clinic Visit: Mrs. Jones Additional history from Mrs. Jones… • Describes having pain with intercourse, especially with insertion • Denies itching or discharge Our patient Normal anatomy
Based on her physical exam findings, what is the most likely cause of her pain with intercourse? • Herpes Simplex Virus • Atrophic vaginitis • Candidiasis
Pain Disorders * Items in red are present in our patient
Causes of Pain Disorders * Items in red are present in our patient
Basic approach to counseling • PLISSIT Model • P: Permission • Normalize certain sexual practices • Li: Limited Information • Educate about normal aspects of arousal • Importance of foreplay • Medication side effects or medical illnesses • SS: Specific Suggestions • Use of topical estrogen, KY jelly, environmental changes • IT: Intensive Therapy • Refer to sex therapy
Summary of Case: Mrs. Jones • Hypoactive Sexual Desire Disorder • Post-partum, breast feeding, “mini-pill” • Relationship issues, stress, depression • Arousal Disorder • Stressed and depressed • On an anti-histamine • Problems with lubrication • Orgasm Disorder • Being treated with an SSRI • Pain Disorder • Atrophic vaginitis
In Summary • Ask about sexual health • Remember that FSD is often multi-factorial • History should address issues of: • Desire, Arousal, Orgasm, Pain • Look for and treat any underlying causes • Recognize psychosocial influences • Opportunity to educate • Refer for therapy when appropriate
References • Frank JE et al. Diagnosis and Treatment of Female Sexual Dysfunction. AFP. Vol 77, no. 5. March 1, 2008: 635-642 • Raina R et al. Female Sexual Dysfunction: classification, pathophysiology and management. Fertility and Sterility. Vol 88, No. 5, Nov 2007: 1273-1284. • Heiman J. Becoming Orgasmic • Lindau et al. A study of sexuality and health among older adults in the United States. NEJM 357;8, 2007: 762-774. • Erdogan A Female Sexual Dysfunction. Int Urogynecol J (2008) 19:293-305 • Lightner DJ Female Sexual Dysfunction. A Concise Review for Clinicians. Mayo Clin Proc. 2002;77:698-702