Download
1 / 30
300 likes | 392 Vues
Discover the evolving role of CHWs in Sub-Saharan Africa, focusing on a program in South Kenyan district. Explore challenges, solutions, and successes faced by CHW programs in addressing public health issues. Presented by Dr. Edwin Lutomia Mangala, this session provides insights into the critical need for support, supervision, and incentives for effective community health work.

E N D
COMMUNITY HEALTH WORK IN SUB-SAHARAN AFRICA: The Kenyan experience The role of CHWs in sub-Saharan Africa has evolved over time and place in response to changing health care priorities, disease burdens, and shortages of human resources for health. CHW programmes play a crucial role in the support and delivery of services in sub-Saharan Africa and are critical in efforts to tackle the existing health worker crisis. However, they need support, supervision and financial and non-financial incentives if they are to carry out their work effectively. This session will look at how one such CHW programme in a South Kenyan district at the foot of Mt.Kilimanjaro informs the above issues. Presented by: Dr. Edwin Lutomia Mangala MSc. Public health-health promotion student Leeds Metropolitan University.
Objectives • To analyse, through a practical example, the role of CHWs in public health in Sub-Saharan Africa • To identify some of the key challenges that face CHW programs • To explore possible solutions to identified challenges
Scope • Background information • Social, political, economic • The healthcare system • The CHW program in Loitokitok district • Design and implementation • Early challenges and intervening measures • Successes and failures • Key issues arising
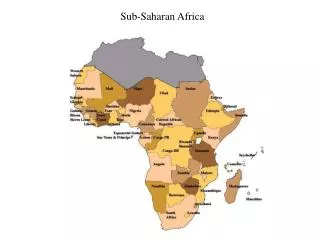
Background • Sub-Saharan Africa & Kenya
Country Profile • Geography • 580,367sq.km • Capital – Nairobi • Other cities – Mombasa, Kisumu • People • Population – 39m • Religion – Christian 82.6%, Muslim 11.2%, Traditional 5% • Languages • Official – English, Swahili • Others – 40 from Bantu (67%), Nilotic (30%) and cushitic (3%) • Government • President • Prime Minister • Economy • Largest in Eastern Africa • Services – 59.5% • Agriculture – 23.8% • Industry and commerce – 16.7% • Political • Multiparty state in 1992 • New constitution 2010 • Over 40 political parties
Kenya health care system • Ministry of Health • Ministry of Medical Services • Ministry of Public Health and Sanitation • Two broad divisions • Public (government owned) • Private
Kenya Healthcare system • Traditional pyramidal structure • Dispensaries and private clinics • Health centres • Sub-district hospitals and nursing homes • District hospitals and private hospitals • Provincial hospitals (8) • National hospitals (2)
Important Institutions • Medical practitioners and dentists board • Clinical officers council • Nursing council of Kenya • Kenya medical supplies agency (KEMSA) • Pharmacy and Poisons Board • National hospital insurance fund (NHIF) • Kenya Medical Research Institute (KEMRI)
Source: WHO (2009) • Budgetary allocation to health fell from 7% (2009/2010) to 6.5%; Target 15%
Some key health/Development Indicators Source: WHO (2009)
Healthcare workers • Specialist doctors • Medical Officers • Clinical Officers • Nurses • Public Health Officers
Major causes of morbidity • HIV/AIDS • Tuberculosis • Malaria • Pneumonia • Respiratory tract infections • Road accidents • Factory accidents • Gastroenteritis • Diabetes mellitus
Key Issues • A largely rural and poor population that has limited access to the formal healthcare system • Inadequate expenditure on health • No universal health financing scheme • Limited health workers; mostly urban based
CHW program in Loitokitok district Location • Kuku Group ranch – 1,500 sq.km • Semi-arid • Average Temp- 30 0 Celsius • 12,000 inhabitants - Maasai Community • Nomadic herders • Traditional
Implementing agencies/Institutions • Ministry of public health and sanitation • Maasai Trust • Christian Children’s Fund • African Medical Research Foundation (AMREF)
Health workers • Public health Officer (1) • Medical Officer (1) • Nurses (6) • Support staff (10)
Structure • CHW selection by community • Training (3 months) • Allocation • 1CHW per 2-3 homesteads (20-30 households) • Duties – Water, sanitation, ITNs, Immunization, Antenatal care, Delivery, nutrition, communicable diseases, health education • Resources – Bicycle, CHW bag, Stationery • Reporting/supervision • Monthly to health centre
Early challenges • Too much workload for CHWs • Motivation • Failure to translate theory into practice ? literacy • Large coverage area
Emergency measures • Reduce number of CHWs • Narrow focus • Closer supervision • Incentives
Notable successes • Increased immunization coverage • Home management of diarrhoea using Oral Rehydration Salts • Surveillance system
Failures • Water and Sanitation • Reproductive health • ITNs
Key Issues • Resource limited setting • Does it increase access? • Does it address health workers shortage? • Cost-effectiveness • Is it really cheap? • Empowering • Who decides? • Who acts? • How is success evaluated
Excerpts from Kenya budget 2011/2012 • £10m – Recruitment of 3,150 nurses and 1,050 public health officers for rural areas • £2.7m – 1,050 motorcycles and 2,100 CHWs in rural areas