Understanding ICD-10-CM Impact on Oncology Operations: Key Insights from the 2011 MPFS
810 likes | 952 Vues
This introduction to ICD-10-CM by Bobbi Buell, MBA, outlines the essential changes and implications for oncology practices following the implementation of the Medicare Physician Fee Schedule (MPFS) in 2011. Emphasizing awareness and operational readiness, it highlights significant aspects such as telehealth services, practice expenses, and reimbursements for biopharmaceuticals. Healthcare professionals can gain insight into navigating the changes in reimbursement structures and patient care practices driven by the new coding system and regulations.

Understanding ICD-10-CM Impact on Oncology Operations: Key Insights from the 2011 MPFS
E N D
Presentation Transcript
ICD-10-CM An Introduction 2011 Bobbi Buell, MBA onPoint Oncology LLC 800-795-2633 bbuell@onpointoncology.cim
Main Objective • Create an awareness of ICD-10-CM. • Start to consider the impact the conversion to ICD-10 will have on your operations. • Start to understand what it means and does not mean in Oncology.
FINAL MPFS 2011 • On November 2, 2010, the Centers for Medicare & Medicaid Services (CMS) posted a proposed notice for Medicare payments in the physician fee schedule for calendar year (CY) 2011. • Many of these provisions were specified in Health Reform (“ACA”). The final rule (CMS-1502-P) affects physicians and office payment for services paid under the resource-based relative value scale/system (RBRVS), also known as, the Medicare Physician Fee Schedule. • Here are the highlights of Rule which becomes effective for dates of service on or after 11-2-2010. https://www.cms.gov/PhysicianFeeSched/PFSFRN/list.asp#TopOfPage onPoint Oncology LLC
FINAL MPFS 2011 • Practice Expense: CMS continues for the second year (at a 50/50 blend), the phasing-in over four years the implementation of the American Medical Association (AMA) Physician Practice Information Survey (PPIS) data administered in 2007/08 for practice expense (PE) indirect per hour rate. Oncology is still using the AMA SMS data series. Of interest is this year's calculation of practice expense for drug administration because many of our codes were bumped up slightly to include some supplies. https://www.cms.gov/PhysicianFeeSched/PFSFRN/list.asp#TopOfPage onPoint Oncology LLC
FINAL MPFS 2011 • Related –TC of Imaging Codes Get Cuts: Well, of course, this is happening in July 2010. But, what it means is that, as of July 6, you will get a cut of 50% for secondary –TCs of related procedures in the same family of imaging procedures. This has been expanded to include more and unrelated procedures. SEE ADDENDUM F of the fee schedule for additional procedure reduction codes. • Telehealth Services: To perform telehealth services, there must be two-way communication between provider and patient, plus you must be in HPSA (Health Provider Shortage) area or outside an MSA. Additional services proposed as allowable in 2011 are 99231-99233 (every three days) and 99307-99310 every 30 days along with services that are unrelated to Oncology. onPoint Oncology LLC
FINAL MPFS 2011 • Physician Extenders: They are sometimes known as NPs and PAs. They can now perform certification and periodic re-certification for SNF patients. • Bone density payment: The proposal calls for these to be paid 70% of the 2006 RVUs at the 2006 conversion factor with this year’s GPCIs for codes 77080-77082. This is retroactive to January 1, 2010. • Payment for Biosimilars: Here is the payment formula for drugs that are ‘similar’ to today’s biologics. Down the road, we will see lots of these in cancer treatment for sure… • A biosimilar is a product approved under an abbreviated application for a license of a biological product that relies on a license of another biologic. • The payment for these biosimilar products will be the sum of all ASPs assigned to a biosimilar products divided by all applicable units plus six percent of the REFERENCE PRODUCT…how does that work? onPoint Oncology LLC
FINAL MPFS 2011 • Self-Referral Disclosure Law: Effective for dates of service after January 1, 2011 for CAT, MRI, and PET: • A list of FIVE (not ten) alternative ‘suppliers’ (not a hospital) within a 25-mile radius of the physician’s office who provide the same imaging services. If there are not five, you must list all. • The list must include, name, address, phone number of other facilities. If there is no one they can go to, tell the patient they can get these tests in other facilities. • The list is to be given to the patient at the time of referral. EACH time the patient is referred it must be given. • No signature or form retention is required. Make a note in the chart or get a stamp for charts---but there should be a notation that it was given. • Must be written in a way that patients can understand. • Emergency situations are not an exception. • Exceptions include patients who are not on Medicare at the time of the referral. onPoint Oncology LLC
FINAL MPFS 2011 • Drugs: This rule maintains the current average sales price (ASP) + 6% reimbursement for Part B drugs; however, it includes proposed changes to ASP reporting, thresholds, and vial amounts. • Among other provisions, if the manufacturer is late with quarterly reporting, the CMS proposes to update ASPs by carrying over the previously reported manufacturer ASP for applicable national drug code(s) (NDC(s)). This is called the “carry over” methodology. This method will not be implemented if there are not a significant number of involved NDCs. But, manufacturers are still subject to Civil Monetary Penalties, if they make a habit of not submitting ASPs. • CMS also proposes to update the regulations to clearly state that Medicare will not pay for amounts of “overfill”, i.e. product in excess of the amount reflected on the FDA-approved label. The ASP plus 6% will be paid for FDA-approved amounts in the vial, but practices may not bill for and/or pool their overfill. • Partial quarter ASPs for new drugs were also discussed in the proposed rule. Single-source drugs will be priced at WAC, plus 6% for that quarter and multisource and line extension drugs will be added to the weighted average of applicable NDCs. • CMS also proposes to maintain the applicable threshold percentage for price substitution of WAMP or AMP for two consecutive quarters at 5%. CMS also finalizes the proposal to maintain the applicable threshold percentage for price substitution at 5%, however did not finalize a new proposal for price substitution at 103% of average manufacturer price (AMP) in certain circumstances when the ASP exceeds the AMP. onPoint Oncology LLC
What is Overfill? • An amount in the vial that is not indicated on the label. • It is an amount not included in what you paid for in terms of vial size. • Under ‘incident to’, practices may not be reimbursed for anything which does not represent an expense to them. • Prior to the final rule, overfill was statutorily excluded from payment. But, the FR reinforced this. onPoint Oncology LLC
FINAL MPFS 2011 • Signature on Requisition: CMS will require a physician’s or a non-physician practitioner’s signature on requisitions for clinical diagnostic laboratory tests paid under the Clinical Lab Fee Schedule. This has gotten very negative comments in the past. • CMS believes that signatures are already required on orders for clinical diagnostic laboratory tests paid under the Clinical Lab Fee Schedule and there is confusion about the difference between an order and a requisition. • The proposed policy will also be consistent with the requirement that orders for diagnostic tests paid under the MPFS must be signed by a physician or appropriate non-physician practitioner. • CMS has updated this policy to state that it will not be enforced First Quarter 2011. There are also very public rumors that this will go away. • One-year filing for Part B claims: There has already been a transmittal about this. But, starting January 1, 2010, there will be a one-year filing deadline for claims. onPoint Oncology LLC
FINAL Fee Schedule 2011 • PQRI for 2011: This year, there are 194 measures in the rule. Like last year, there are 2 reporting periods: 6 months and 12 months. Other proposed changes to PQRI applicable to office-based cancer practices include: • Registries: CMS once again emphasized that Registries are the way to go for more accuracy in PQRI data submission. CMS wants to get away from claims submissions ASAP. New cancer registry: pqri@unlimitedsystems.com. • Success Criteria: It is PROPOSED for claims ONLY that you report on at least 3 measures (if applicable) AND you report on at least 50% of applicable patients, instead of 80%---which would still be the rate for EMR/EHR or Registry submission. • Group Practices: Two types of group practices are proposed to report in 2011. First are practices over 200 eligible providers called GPROI. Then there are groups 2-199 eligible providers called GPROII. To report as a GPROII, you must self-nominate; be in the first 500 practices to do so after the beginning of the year 2011; and, you must report at least one of GPROII groups, which do not apply to many cancer practices. CMS is looking for specialty measures groups for GPROII. • Deleted Measures: These measures used by cancer folks are leaving (maybe) in 2011: • Measures 114 and 115 for Tobacco Use (more later about this); • Measure 136 for Melanoma • Measures Reportable by Registry Only: These are the same as last year: • 137-138: Melanoma • 143-144: Pain In Cancer Measures onPoint Oncology LLC
FINAL E-Prescribing 2011 • E-Prescribing: E-prescribing will pay 1% of the providers’ billed and allowed fee schedule services (all services paid by RVUs) in 2011. 2011 is the last year where you will not be penalized, if you do not participate if you qualify. BUT, 2011 is the year that those that should be penalized will be identified. The penalty only exists for those who do not have at least 100 cases in the denominator codes (mostly E/M); who do not report at least 10 encounters by mid-2011, or, do not qualify as a physician or physician extender who has at least 10% of fee schedule revenue in the denominator codes. https://www.cms.gov/PhysicianFeeSched/PFSFRN/list.asp#TopOfPage onPoint Oncology LLC
E-Rx Reporting • For successful claims-based reporting in 2011,a single code should be reported (numerator) G8553 – At least one prescription created during the encounter was generated and transmitted electronically using a qualified e-Rx system • Must be on the same claim (denominator)–90801, 90802, 90804, 90805, 90806, 90807, 90808, 90809, 90862, 92002, 92004, 92012, 92014, 96150, 96151, 96152, 99201, 99202, 99203, 99204, 99205, 99211, 99212, 99213, 99214, 99215, 99304, 99305, 99306, 99307, 99308, 99309, 99310, 99315, 99316, 99324, 99325, 99326, 99327, 99328, 99334, 99335, 99336, 99337, 99341, 99342, 99343, 99344, 99345, 99347, 99348, 99349, 99350, G0101, G0108, G0109 • Combination is reported on at least 25 encounters onPoint Oncology LLC
FINAL E-Prescribing • If you participate in the HIT incentive, you may not receive the e-prescribing incentive, but you must e-prescribe AND FOR NOW YOU MUST REPORT! • Incentive • Reporting period: Calendar year, but data 1/1/2011-6/30/2011 will be used to identify those who should be penalized. So, you must report at least 10 encounters per NPI before 6/30/11. • Reporting mechanisms: CLAIMS ONLY!! • Hardship exceptions—there will be new G-codes for these: • Rural practices with no high speed internet OR • Providers near pharmacies that do not process e-rx. onPoint Oncology LLC
Hospital Outpatient PPS 2011 • Drug payments– Continue standard packaging methodology for drugs under a certain benchmark. • Drugs costing less than $70 per day are packaged into ambulatory payment classification (APC) • Drugs costing more than $70 are reimbursed separately • Separately billable drugs paid at ASP+5% • Only 5-HT3 antiemetic product exempt from standard packaging methodology is palonosetron hydrochloride—used to be all 5 HT-3s onPoint Oncology LLC
HOPPS 2011 • Ongoing discussion about supervision requirements • Under direct supervision CMS clarified that supervising physician or non-physician practitioner (NPP) must be “immediately available”– CMS not defining “immediately available” but referenced as physically present and interruptible. • Varies by type of facility. onPoint Oncology LLC
HOPPS 2011 • In the New Rule • Commencing in 2010, CMS allows certain non-physician practitioners (NPPs) – example, PAs, NPs, clinical nurse specialists – to provide direct supervision for hospital outpatient therapeutic services they are authorized to perform in state scope of practice rules and under hospital privileging. Chemo requires direct supervision; other drug administration does not • For an on-campus hospital outpatient setting the rule is met by immediate availability of either a physician or NPP anywhere on the same hospital campus and immediately available to furnish assistance and direction throughout performance of the procedure (may be in non-hospital space on the campus) • For an off-campus outpatient department, supervising physician or NPP must be in the provided-based department (though not necessarily in the same room)
FOUR BIG-TIME INITIATIVESWILL BEGIN OR HAVE BEGUN THIS YEAR Is Your Organization Prepared?
I.A. Beginning in October 2010* 2009 ARRA / HITECH Act Medicare / Medicaid Incentive Payments MEANINGFUL USE of CERTIFIED EHRs Providers / Hospitals • Division B, Title IV: Electronic Health Record (EHR) Installations Incentive Payments are for “Adoption and Meaningful Use of Certified EHR Technology” *Applies to Medicare ONLY – US Hospitals
I.B. Began in February 2010* 2009 ARRA / HITECH Act HIPAA “TWO” Confidentiality/ Privacy and Security Standards • Division A, Title XIII - Subtitle D: 1996 HIPAA Title II--Administrative Simplification Standards Modifications • The Confidentiality and Privacy Standards • The Security Standards *HHS’ OCR begins to enforce Privacy Rule only after a rule is in place; Privacy’s Breach Rule already in place Applies to ALL (new / existing) HIPAA CEs
II. Compliance on January 1, 2012 1996 HIPAA Title II--Administrative Simplification Standards Modifications • The EDI Transactions Set Version 5010 and D.0 Transactions Applies to ALL (new / existing) HIPAA Covered Entities and ALL Accredited Standards Committee (ASC) X12 and National Council for Prescription Drug Program (NCPDP) transactions
HIPAA 5010 COMPLIANCE DATES • HIPAA 5010 EFFECTIVE DATE: March 17, 2009 • LEVEL I COMPLIANCE BY: December 31, 2010 • CMS Medicare Fee-for-Service Schedule: April 1, 2010 through December 31, 2010 • LEVEL II COMPLIANCE BY:December 31, 2011 • CMS Medicare Fee-for-Service Schedule: January 1, 2011 through December 31, 2011 • ALL CEs FULLY COMPLIANT ON:January 1, 2012
Beginning on October 1, 2013 ICD-10-CM / PCS Physician Behavioral Health Hospital ICD-10-CM CPT / HCPCS ICD-10-CM CPT / HCPCS ICD-10-CM ICD-10-PCS Inpatient ICD-10-CM CPT / HCPCS Laboratory All Other Outpatient ICD-10-CM CPT / HCPCS ICD-10-CM CPT / HCPCS Long Term Healthcare ICD-10-CM CPT / HCPCS
Why is ICD-9 Being Replaced? • ICD-9-CM is out of date and running out of space for new codes. • Lacks specificity and detail • No longer reflects current medical practice • ICD-10 is the international standard to report and monitor diseases and mortality, making it important for the U.S. to adopt ICD-10 based classifications for reporting and surveillance. • ICD codes are the core elements of HIT systems, conversion to ICD-10 is necessary to fully realize benefits of HIT adoption.
Coding Process Remains the Same • ICD-10-CM code book retains the same traditional format • Index • Tabular • Process of coding is similar • Look up a condition in the Index • Confirm the code in the Tabular
Comparison of ICD-9-CM and ICD-10-CM ICD-9-CM CODE ICD-10-CM CODE A - Category of code B - Etiology, anatomical site, and/or severity C - Extension 7th character for obstetrics, injuries, and external causes of injury • A - Category of code • B - Etiology, anatomical site, and manifestation A A B C B
ICD-9-CM Structure – Format Numeric or Alpha (E or V) Numeric X V 5 E 4 X 1 X 4 X 0 0 X . . Category Etiology, Anatomic Site, Manifestation 3 – 5 Characters
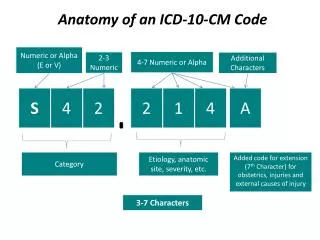
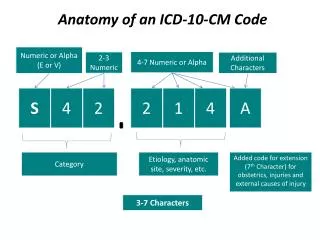
ICD-10-CM Structure – Format Alpha (Except U) Additional Characters 2 - 7 Numeric or Alpha . . X X X A M A X S 3 X 2 X X 0 1 0 Added code extensions (7th character) for obstetrics, injuries, and external causes of injury Category Etiology, Anatomic Site, Severity 3 – 7 Characters
Comparison of ICD-9-CM and ICD-10-CM Codes: 707.0 Pressure ulcer 707.00 - unspecified site 707.01 - elbow 707.02 - upper back 707.03 - lower back 707.04 - hip 707.05 - buttock 707.06 - ankle 707.07 - heel 707.09 - other site Code Examples: L89.131 – Pressure ulcer of right lower back, stage I L89.132 – Pressure ulcer of right lower back, stage II L89.133 – Pressure ulcer of right lower back, stage III L89.134 – Pressure ulcer of right lower back, stage IV L89.139 – Pressure ulcer of right lower back, unspecified stage L89.141 – Pressure ulcer of left lower back, stage I L89.142 – Pressure ulcer of left lower back, stage II L89.143 – Pressure ulcer of left lower back, stage III L89.144 – Pressure ulcer of left lower back, stage IV L89.149 – Pressure ulcer of left lower back, unspecified stage L89.151 – Pressure ulcer of sacral region, stage I L89.152 – Pressure ulcer of sacral region, stage II … L89.90 – Pressure ulcer of unspecified site, unspecified stage
New Features of ICD-10-CM • Combination codes for conditions and common symptoms or manifestations • Combination codes for poisonings and external causes • Added laterality • Expanded codes: injury, diabetes, alcohol/substance abuse, postoperative complications
New Features of ICD-10-CM • Added extensions for episode of care • Inclusion of trimester in obstetrics codes and elimination of fifth digits for episode of care • Expanded detail relevant to ambulatory and managed care encounters • Inclusion of clinical concepts that do not exist in ICD-9-CM • Changes in timeframes specified in certain codes
Useful in Cancer?? • Laterality – Left Versus Right • C50.1 Malignant neoplasm, of central portion of breast • C50.111 Malignant neoplasm of central portion of right female breast • C50.112 Malignant neoplasm of central portion of left female breast
Useful In Cancer??? • ICD-9-CM • 143 Malignant neoplasm of gum • 143.0 Upper gum • 143.1 Lower gum • ICD-10-CM • C03 Malignant neoplasm of gum • C03.0 Malignant neoplasm of upper gum • C03.1 Malignant neoplasm of lower gum
What are GEMs? • “GEMs” stands for General Equivalence Mappings • The CMS and the CDC created GEMs to ensure consistent national data when the U.S. adopts ICD-10. • The GEMs will act as a translation dictionary to bridge the “language gap” between the two code sets and can be used to map an ICD-9 code to an ICD-10 code and vice versa.
Purpose of GEMs • Designed to give all sectors of the healthcare industry that use coded data the tools to: • Convert large databases and test system applications • Link data in long-term clinical studies • Develop application-specific mappings • Analyze data collected before and after the transition to ICD-10-CM
Not a Substitute for Coding • The GEMs should not be used as a substitute for learning how to use the ICD-10-CM code sets. • “GEMs are not a substitute for learning ICD-10-PCS and ICD-10-CM coding. They’ll help you convert large data sets.” • Mapping simply links concepts in the two code sets, without consideration of context of specific patient information, whereas coding involves assigning the most appropriate code based on documentation and applicable coding guidelines.
Why a GEM Won’t Always Work • A clear one-to-one correspondence between an ICD-9 or ICD-10 code is the exception rather than the rule. • ICD-9 codes: 414.01 Coronary atherosclerosis of native coronary artery and 411.1 Intermediate coronary syndrome (unstable angina) • ICD-10 code :I25.110 Atherosclerotic heart disease of native coronary artery with unstable angina • There are situations when a code in the target system does not exist • T503x6A Underdosing of electrolytic, caloric and water-balance agents, initial encounter
Forward and Backward Mapping Forward Mapping Backward Mapping
ICD-10 Implementation Plan Checklist: http://www.ahima.org/icd10/ICD-10PreparationChecklist.mht Year 2009/ 2010 2011 2012 2013 Phase I Awareness and ImpactAssessment Phase II Preparing for Implementation Phase III Go Live Preparation Phase IV Post – Implementation
Clinical Documentation • The increased specificity of the ICD-10 codes requires more detailed clinical documentation in order to code some diagnoses to the highest level of specificity. • There are “unspecified” codes in ICD-10-CM for those instances when medical record documentation is not available to support more specific codes. • The benefits of ICD-10 can not be realized if non-specific codes are used rather than taking advantage of the specificity ICD-10 offers.
Improving Documentation • Conduct medical record documentation assessments • Evaluate records to determine adequacy of documentation to support the required level of detail in new coding systems • Implement a documentation improvement program to address deficiencies identified during the review process • Educate providers about documentation requirements for the new coding system through specific examples • Emphasize the value of more concise data capture for optimal results and better data quality