Download
1 / 34
340 likes | 837 Vues
Measles and Neonatal Tetanus: Clinical Signs and Treatment. Measles and Neonatal Tetanus: Clinical Signs and Treatment. Prof. Pushpa Raj Sharma Institute of Medicine Kathmandu . Measles Case definition.

E N D
Measles and Neonatal Tetanus: Clinical Signs and Treatment Measles and Neonatal Tetanus: Clinical Signs and Treatment Prof. Pushpa Raj Sharma Institute of Medicine Kathmandu
Measles Case definition • Laboratory confirmation in the absence of recent immunization (1-14 days) with measles containing vaccine: • Detection of measles virus from urine or throat/nasopharyngeal swabs or • Significant rise in the measles antibody titre between acute and convalescent sera or • Positive serologic test for measles IgM antibody using a recommended assay.
Measles: Basic Characteristics • Also known as “dadura”/”bhosa kai” / rubeola / fourth day disease/ first fever • Acute viral illness • Primarily affects children • Highly contagious • Paramyxovirus • RNA, single stranded • Vaccine preventable • Potential to be eliminated
Measles: Signs and Symptoms • Incubation period: 10-12 days (8-16 range) • Prodrome • Cough • NP, worsens over 4 days, then improves • Lasts through entire illness (7-10 days) • Conjunctivitis (purulent), coryza • May include photophobia • Lasts 6-8 days • Fever: 38-40o C: subsides after 1 week • Diarrhea • Chronic, serious if previously malnourished
Measles: Signs and Symptoms • Koplik’s spots • Part of prodrome: day 1-3 before rash • Raised papules on buccal mucosa and conjunctiva • Usually adjacent to molars • Often white on red base • Disappear about time rash occurs
Erythematous papular eruption Travels inferior over 2-3 days Coalesces into macular “splotches” Often desquamates at end of illness Measles: Signs and Symptoms Rash Hairline Behind Ears Face Trunk Limbs
Measles: Signs and Symptoms • Peak of Illness • 2-4 days after onset of rash • Other signs and symptoms • Anorexia, malaise, hemorrhagic, • Resolution • Rapid improvement at end of febrile period (1 week) • Complete recovery in 10-14 days
Summary: Diagnosis / Clinical • Clinical illness includes all of the following symptoms: • Temperature of 38.3°C or more. • Cough, coryza or conjunctivitis • Generalized maculopapular rash for at least three days following temperature and cough, coryza or conjunctivitis. • Koplik’s spots can be classic, but easily missed
Measles Dengue Enteroviruses Rubella Kawasaki MaculopapularRash with Fever Scarlet Fever Echoviruses Reoviruses Mononucleosis Roseola Infantum
Low grade fever, headache and mild URI symptoms Erythematous facial flushing. “Slapped cheek appeaarence
High fever for three days. Developed generalized seizure on the third day. No specific localizing signs. Investigations including LP normal Developed rash on the fourth day after the fever subsided. Rash first appeared on trunk sparing palm and sole
Presented with Jaundice and drowsiness, ascitis Started ampicillin Developed rash on 4th day.
Bilateral periorbital edema not associatedwith generalized edema Maculopapular rash Fever and rash for three day Forehead and cheeks flushed Non itchy, maculo-papular, punctate, granular generalized, first noticed over neck.
Mild fever and cough for two days Developed rash on the second day of fever which appeared on face first and spread allover in one day. Fever: 99.2 axillary; enanthem on the soft palate; tender discrete lymph nodes over retro auricular, sub occipital and posterior cervical region. Rash cleared on third day.
Exanthem a common clilnical manifiestation Nonspecific febrile illness (no coryza and conjunctivitis) Rubeolliform rash Rash and fever same time Rash last 3-5 days
Five years , child moderate fever, a hacking cough, runny nose, red eyes for three days. On examination enanthem was present on the hard and soft palate. Grayish white dots were seen opposite the lower molars. On fourth day temperature: 104ºF. Faint macules on the upper lateral parts of neck, behind the ears, along the hair line, and on the posterior parts of neck was noticed. Case history:
Major Complications • Acute Post-infectious Encephalitis • Occurs in 1-4/1000, 2-6 days after rash • Mild to fulminant (death in 24 hours) • 25% morbidity; 15% mortality • Subacute Sclerosing Panencephalitis–SSPE • 2-15 years after infection • Progressive behavioral changes • Secondary infections: Pneumonia; flaring of tuberculosis. • Myocarditis • Corneal ulcer
Measles: Prognosis • Mortality varies by age / nutritional status • Historically 1-5% • Higher with close contact secondary cases from presumed high viral exposure • West Africa/Asia: 25% • Death: pneumonia, malnutrition, diarrhea • Risk factors • Immune compromise, Vitamin A deficiency
Measles: Treatment • Supportive Care • Rest, hydration, nutrition, prn meds • Look for and treat bacterial super-infections • Rinse eyes daily (saline or sterile water) • Vitamin A • May decrease mortality by 40% • Benefit may be independent of deficiency • WHO recs for both hospitalized and less ill • Ribavirin • Inhibits viral replication in cell culture • Limited benefit in immune compromised patients • High cost makes = impractical in developing world
Measles: Treatment* *WHO Recommendations
Some Myths • Over clothing is essential. • Do not use antipyretics. • Do not give meat / egg / fruits / oil. • Keep in a room with windows closed. • Religious Puja. • Herbal medicines in eye. • My child has three episodes of measles within one year.
Measles: Prevention • Maternal antibodies • Protect for 3-12 months; usually 6 months • Presence of Ab’s makes vaccine less effective • Passive Immunization • Gamma globulin (0.25mg/kg) • For: high risk pts and exposure within 6 days • Pregnant, immune suppressed, children too young for vaccine, active TB, leukemia, known HIV • Impractical for developing world
Measles: Prevention • Vaccine Immunization • Live attenuated vaccine • Efficacy (seroconversion) • Lifelong immunity • 9 months: 80-85% • Second dose with MMR at 16 months: >90% • Contraindications (live vaccine) • Immune suppressed, leukemia, lymphoma, pregnancy, anaphylaxis to neomycin or gelatin • Most recommend vaccinating HIV patients
Measles: Prevention • Vitamin A • National Vit. A programme • Targets children >= 6 months old • Decrease mortality by improving nutrition • Benefit likely involves many infections, but measles is at the top
Neonatal Tetanus • First described by Hippocrates • Etiology discovered by Carle and Rattone in 1984 • Passive immunity used for treatment and prophylaxis during World War I • Tetanus toxoid first widely used during World War II
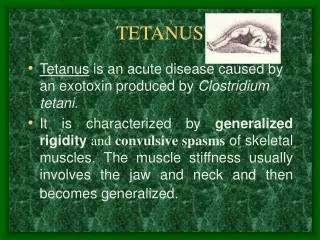
Tetanus Pathogenesis • Anaerobic condition helps to germinate spores and production of toxins. • Toxins binds to the central nervous system • Interferes with the neurotransmitter release to block inhibitory impulses. • Leads to unopposed muscle contraction and spasm.
Clinical Features • Incubation period: 8 days (3-21 days). • Three clinical forms: • Local (not common) • Cephalilc (rare) • Generalised most common • Descending symptoms of trismus, difficulty swallowing, muscle rigidity and spasm. • Spasm continues ( consciousness retained)
Neonatal tetanus A conscious spasm
Tetanus: complications • Laryngospasm • Hypoglycemia • Nosocomial infections • Myoglobinuria • Aspiration • Iatrogenic apnoea • Death
Management: Principles • Eradication of C. tetani. • Penicillin G 100,000 U / kg / 24 hrs. • Neutralizing the toxin • Human tetanus immunoglobulin: 500 IU IM • TAT: 10,000 – 100,000 U (I/2 IM and ½ IV) • Prevent spasm: • Diazepam: 0.1 – 0.2 mg every 3 – 6 hourly intravenously. • Dantrolene; chlorpromazine; baclofen • Vecuronium and pancuronium with Mechanical ventilation (best survival rate)
Management: contd. • IV line. • Nasogastric tube feeding. • Minimal handling. • A separate room.
Prevention • An entirely preventable disease • Mortality <10% (intensive care treatment) > 70% without intensive care treatment. • Antenatal Tetanus Toxoid
Thank you www.prsharma.com.np