Gastroenterology
Gastroenterology. Swedish Family Practice Residency Didactics July 31, 2001. A quick trip through the GI track with brief stops at the esophagus, stomach, liver, colon, rectum and anus. And a little diarrhea. The Upper GI Tract. Esophagus Stomach Pancreas Gallbladder Liver.

Gastroenterology
E N D
Presentation Transcript
Gastroenterology Swedish Family Practice Residency Didactics July 31, 2001
A quick trip through the GI track with brief stops at the esophagus, stomach, liver, colon, rectum and anus.And a little diarrhea.
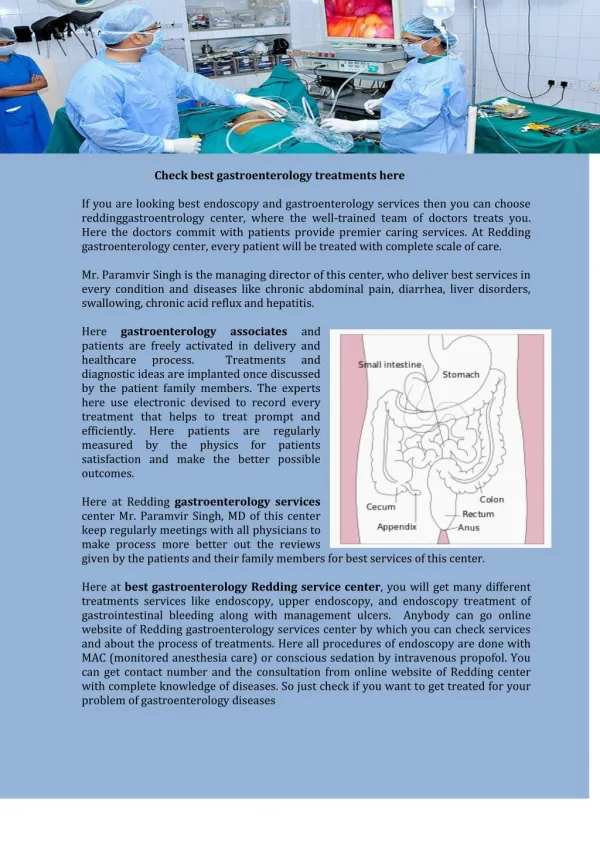
The Upper GI Tract • Esophagus • Stomach • Pancreas • Gallbladder • Liver
Esophageal Disorders • Disorders of motility • GERD • Inflammatory and infectious disorders • Tumors
Symptoms from the Esophagus • Dysphagia • Odynophagia • Chest pain • Regurgitation
Disorders of Motility • Achalasia – Cancer, Parkinson’s, Chagas Disease (trypanosomiasis) • Spasm – Diffuse, Localized • Scleroderma
Diagnostic Studies • Barium swallow • Manometry
Treatment • Long-acting nitrates • Calcium channel blockers • Dilation of LES (Achalsia) • Surgery (Spasm, Scleroderma) • Manage reflux (Scleroderma) • Prokinetic drugs (Scleroderma)
GERD • Frequent – 10% of US population • Occasional – 30% of US population
Symptoms of GERD • Heartburn • Water Brash • Regurgitation • Dysphagia/odynophagia • Chest pain, hoarseness, chronic cough, wheezing
Diagnosis of GERD • Therapeutic trial • Endoscopy (if complicated) • Manometry (for placement of pH probe or prior to reflux surgery) • pH acid perfusion test (for diagnosis of unresponsive GERD)
Treatment of GERD Mild Symptoms • Dietary modification • Lifestyle modification • Trial of patient directed therapy with OTC antacids or H2 antagonists
Treatment of GERD Non-responders, non-erosive disease • H2 antagonists • PPI’s • Promotility agents • 8-12 weeks of therapy
Warning Symptoms Suggesting Complicated GERD • Dysphagia • Bleeding • Weight loss • Choking (acid causing coughing, shortness of breath , or hoarsness) • Chest pain • Longstanding symptoms requiring continuous treatment
Treatment of GERD Complicated GERD • GI workup with endoscopy • PPI’s • High-dose H2 antagonists • Antireflux surgery – no data on new procedures
Inflammatory Disorders of the Esophagus • Pill-induced esophagitis – NSAID’s, steroids, doxycycline • Infective esophagitis – HIV, HSV, cytomegalovirus, candida • Corrosive – alkalis or acids
Diagnosis and Treatment Endoscopy Treatment based on results of endoscopy
Esophageal Tumors • 90% are malignant • Most are squamous cell • Most are associated with heavy alcohol and tobacco use • 8% of Barrett’s develop into adenocarcinomas • 5% 5-year survival but improving
Diseases of the Stomach • Acid peptic disorders of the stomach and duodenum • Infections • Motor disorders • Cancer
Acid Peptic Disorders • 5 – 10% of the US population will have PUD in their lifetime, 50% will recur • .0001% mortality rate
Cause of PUD Imbalance between protective and aggressive factors
Protective factors • Mucus and bicarbonate secretion of epithelial cells • Surface membrane of mucosal cells • PG E-1 and PG E-2
Gastic acid NSAID’s Corticsteroids Smoking Alcohol (?) Stress (?) Diet (probably not) H-pylori Aggressive Factors
H. pylori and PUD • Almost all patients with H. pylori have antral gastritis • Eradication of H. pylori eliminates gastritis • Nearly all patients with DU have H. pylori gastritis • 80% of patients with GU have H. pylori gastritis
H. Pylori Diagnosis • Serology ($20-$200) – 90% sensitive, 95% specific – not good for following treatment • Biopsy ($250) – 98% sensitive – 98% specific • Urea breath test ($80-$100) – 95% specific, 98% specific – can be used to document eradication • Stool antigen test ($100-$150) – 90% sensitive, 95% specific – can be used to confirm eradication
Natural History • 20 – 50% heal untreated • 80% heal in 4 weeks of treatment • 75% recur in 6 – 12 months • More recur in patients with H. pylori, smokers, NSAID users • Milk and tobacco slow healing
Treatment of PUD • H2 blockers - $25 a month for generics • Maintenance dose same as treatment dose • 20% recur on maintenance vs. 70% on no treatment • PPI’s - $125 a month (Prilosec soon out in generic)
Treatment of H. pylori • No therapy is 100% • Treatment markedly decreases recurrences of DU • Use of H2 blockers and PPI’s increases eradication rate and hastens relief of symptoms • PPI’s have intrinsic in vivo activity against H. pylori
Diseases of the Lower GI Tract • Constipation – 2% of US population report chronic constipation • Irritable bowel syndrome – a diagnosis of exclusion (CBC, colonoscopy, stool O&P, lactose difficiency, endoscopy)
Diseases of the Lower GI Tract, cont. • Malabsorption – long differential (consider if weight loss, muscle wasting, hair loss, malnutrition) • Inflammatory bowel disease – UC and Crohn’s disease • Mesenteric vascular disease
Diseases of the Lower GI Tract, cont. • Diverticulosis (90% have no symptoms) • Diverticulitis (infectious) • Infectious diarrhea
Diagnosis of Infectious Diarrhea - History • Work • Travel • Eating • Ill contacts • Recent antibiotics • HIV or immunocompromised
Treatment of Mild Symptoms • Maintain hydration: sports drinks, diluted fruit juices, watery soups, pedialyte, WHO formula, IV fluids • Solids as tolerated but avoid milk and milk products
Diagnosis of Infectious Diarrhea • Stool C&S, O&P (x1), fecal blood and leukocytes if no improvement in 48 hours or severe disease with bloody stools, fever, dehydration • Consider sigmoidoscopy
Treatment Pathogens requiring treatment – shigella, giardiasis, E. coli, pseudomembranous entercolitis, V. cholera
Treatment Pathogens that may require treatment – campylobacter, salmonella, amebiasis (5% carriage rate in the US, many are not pathogenic)
Treatment • Most viral and bacterial causes of diarrhea resolve without treatment • Antibiotics may prolong or worsen diarrhea
Diseases of the Lower GI Tract, cont. • Cancer – small bowel (rare), colon (6% incidence) • Anorectal diseases – cancer, hemorrhoids, pruritis ani, fissures • And hepatitis