Download
1 / 56
831 likes | 2.23k Vues
Demineralization and remineralization processes in enamel. Prof. d-r R. Kabaktchieva - 2014. In 1890 W. D. Miller , an American dentist teaching in Germany , published his chemico - parasitic theory of caries

E N D
Demineralizationandremineralizationprocessesinenamel Prof. d-r R. Kabaktchieva- 2014
In 1890 W. D. Miller, anAmericandentistteachinginGermany, publishedhischemico-parasitictheoryofcaries • Millerbelievedthatextractionofthelimesaltsfromtheteethwas a resultofbacterialacidogenesis • Miller'sworkfailedtoidentify dentalplaqueasthesourceofthebacteriaandthebacterialacids It wasthefirststepindentaldecay
G. V. Black, describedthegelatinousmicrobialplaqueasthesourceoftheacids.
Dentalcariesis a multifactorialdiseaseprocess, oftenrepresentedbytheinterlockingcircles Influence of MO, carbohydrates over time
Theremustbe a susceptibletoothandhost; (2) Cariogenicmicroorganismsmustbepresentin a sufficientquantity; (3) Theremustbefrequentexcessiveconsumptionofrefinedcarbohydrates; (4) Thisprocessmustoccurover a sufficientlylongperiodoftime. Forcariestodevelop, 4conditionsmustoccursimultaneously:
When a toothcoveredwithcariogenicbacteriaisexposedto a suitablesubstrate, suchas a refinedcarbohydrate, = • Iftheseconditionspersistover a sufficientlylongperiodoftime thebacteriaproduceacid. anincipientlesiondevelops
Theincipientlesionistheinitialstageoftoothdecaythathasnotpenetratedtheoutersurfaceofthetooth. • Thelesionlookslike a whitespotontheenamel. incipientlesion caries
PhysicalandMicroscopicFeaturesofIncipientCaries • The incipient lesion in her earliest stage, is characterized by • These changes include demineralization histological changes of the enamel which represents the loss of calcium and phosphate and other ions from the enamel
PhysicalandMicroscopicFeaturesofIncipientCaries • Thesecondstageincludestheprogressofdemineralization • Thefinalphaseofcariesdevelopmentisthedevelopmentoftheopen or visible lesion that is actually a really cavitation towardthedentinoenameljunction (DEJ), thencontinuesintothedentin. We can also sayovert, orfrank, lesion
Theearlyidentificationoftheincipientlesionisextremelyimportant,Theearlyidentificationoftheincipientlesionisextremelyimportant, • becauseitisduringthisstagethatthecariousprocess canbearrestedorreversed!!!
The incipient lesion is macroscopicallyvisible on the tooth surface by the appearance of an area of opacity, the white spot lesion. • Atthisearliestclinicallyvisiblestage, thesubsurfacedemineralizationatthemicroscopicleveliswellestablished.
TheincipientlesionhasbeenextensivelystudiedandisbestdescribedbySilverstone.TheincipientlesionhasbeenextensivelystudiedandisbestdescribedbySilverstone. • Тheobservationsoftheincipientlesionhavebeenbasedontheuseof a polarizingmicroscope.
Thismicroscopepermitsprecisemeasurementsoftheamountofspace, calledporespace, whichexistsinnormalenameland toa greaterextentinenameldefects.
If demineralizationprogresses • incontrast, duringremineralization, moreporespaceoccurs; lessporespaceispresent.
DirectConnectionoftheBacterialBiofilmtotheBodyoftheLesion • Toothenamelis composedofinterlockingstructurescalled enamelrods, whichcontain billionsofcrystals. • Theporespresentbetween thecrystalsandtherods form a networkofchannelsthatallowdiffusionoffluid, ionsandsmallmoleculesfoundintheenamel
ThestriaeofRetziusextendthisnetworkintodeeperlayersoftheenamel.ThestriaeofRetziusextendthisnetworkintodeeperlayersoftheenamel.
Diagramof a trichotomizedlesion(gointhreedirections) attributabletodiffusionofacids: • inbothdirectionsundertheenamel • directlyintothebodyofthelesioninthedentin. • T, translucentzone; • B, bodyofthelesion; • R, reactionarydentin; • P, pulp. • (FromSilverstone L. M., & Hicks, M. J. (1985).
, • - • all of them continually changing.
Anychemicalchangesintheplaquecansoonbereflectedthroughouttheenamelanddentinaspartoftheincipientlesion.Anychemicalchangesintheplaquecansoonbereflectedthroughouttheenamelanddentinaspartoftheincipientlesion.
Theinitialacidattackpreferentially : • followedbyremovalof:
Theunderminedsurfacezonecollapses. • Atthesametime, themoresolubleproteinsarelostfromthesubsurfacematrix.
CariogenicBacteria • As a generalrule, thecariogenicbacteriametabolizesugarstoproducetheenergyrequiredfortheirgrowthandreproduction. • Thebyproductsofthismetabolismareacids,whicharereleasedintotheplaquefluid. • Thedamagecausedby MS ismainlycausedbylacticacid, althoughotheracids, suchasbutyricandpropionic, arepresentwithintheplaque.
MeasuringPlaquepH, theStephanCurve • Thereis a continuouspHchangeintheplaqueeverytimefoodisconsumed. • ThereisanalmostimmediatedropinpHwhensugarorsugarysnacksareeaten, followedby a longerrecoveryperiodthanwhenotherfoodsareeaten.
Thisdrop-and-recoverycurvehasbeentermedtheStephancurve; • Differentindividualshavedifferentcapabilitiestobufferacidproduction (see next fig.); • Studieshaveidentifiedfoodsthatareaccompaniedby a dropthecriticalpHof 5.5 to 5.0, suchasdriedfruits, whitebread, cereals, starchyfoods
Fig. Stephancurves. ThesecurvesshowthetypicalplaquepHresponsetoanoralglucoserinse. AnimmediatefallinthepHisfollowedby a gradualreturntorestingvaluesafterabout 40 minutes. Theuppercurvewasobtainedfrommilkandtheloweronefromanapple- drink, showing a largedifferenceintheacidogenicityofthesetwodrinks.
TheRelationshipofSaturationtopH • Theconcentrationofcalciumandphosphateionsintheplaquefluidbathingthetoothattheplaque-toothinterfaceisextremelyimportant becausethesearethesameelementsthatcomposethehydroxyapatitecrystalfoundintheenamel. Ifthefluidadjacenttothetoothissupersaturatedwithcalciumandphosphateionsat a givenpH, theenamelcannotundergodemineralization.
Thesalivaincontactwiththeteethisnormallysupersaturatedwithcalciumandphosphate, comparedwiththelevelsofthesemineralsinenamel. • Thebacterialplaquecanconcentratetheseionstoanevengreaterextent. Forinstance, thenumberofcalciumandphosphateionsinplaqueis 3 timesgreaterthanthenumberinthesaliva.
Thisincreasedconcentrationisofpracticalimportancebecausecalciumandphosphatelevelstendtobeinverselyrelatedtothecariesscore.Thisincreasedconcentrationisofpracticalimportancebecausecalciumandphosphatelevelstendtobeinverselyrelatedtothecariesscore.
AsthepHdropsinanacidattack, thelevelofsupersaturationalsodrops, andtheriskofdemineralizationincreases. ThereisnoexactpHatwhichdemineralizationbegins, only a generalrangeof 5.5 to 5.0.
Demineralizationis a functionofboth: • a dropinpH, • thelengthoftimethattheenamelsurfaceisexposedtotheacidicenvironment. • Differentplaqueshave: • differentinitialpHs, • differentbufferingpotentials, • differentconcentrationsofcalciumandphosphateindifferentpartsofthemouth. A changeinanyofthesevariables resultsin a differentlevelofsupersaturationinthetoothenvironment.
DemineralizationandRemineralizationPrinciples • Demineralizationiscausedbyplaqueacids, whichdissolvethetoothmineralsmakingupthebasiccalcium, phosphate, andhydroxylcrystalsoftheenamel, dentin, andcementum. • Remineralization, requirestheavailabilityofthesameions, preferablywithfluorideas a catalysttoreconstructthemissingordamagedrods, a processthattenCatecallednon-restorativerepair.
Thecrystalsandfluoridecompoundofmostdentalinterestinthedemineralizationandremineralizationprocessare:Thecrystalsandfluoridecompoundofmostdentalinterestinthedemineralizationandremineralizationprocessare: • hydroxyapatite (HAP), • fluorhydroxyapatite (FHA), • calciumfluoride (CaF2).
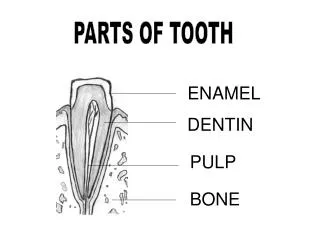
Enamel mineral • The mineral of enamel is a salt formed from calcium phosphates. • Basic calcium phosphate in enamel is hydroxyapatite.
Enamel mineral • Apatite - a mineral with chemical formula Са10(РО4)6 (F, OH)2 • FHA- Ca10(PO4)6(F,OH)2 • FA Ca10(PO4)6 F2
Enamel mineral Other calcium phosphates: Brushite -СаНРО4.2Н 2О, ß-tricalcium phosphate- Са 3(РО 4) 2 Octacalcium phosphate- Са 8(РО 4) 4(НРО 4) 2.5Н 2О.
Dissociation equilibrium of hydroxyapatite НА in liquid medium undergoes electrolytic dissociation HA dissociates to : 10 calcium ions 6 trivalent phosphate ions 2 hydroxide ions Са 10(РО 4) 6 (ОН)2 ←→ 10Са 2+ + 6РО43- + 2ОН -
Calcium and phosphate ions from the enamel get into plaque : - serve for buffering of the medium; • - if the environment is alkaline the iones can reenter in enamel; - part of the ions get into the saliva,
Processes of de-and remineralization of enamel in the oral environment • Between enamel and saliva is situated the plaque biofilm Ions entering the food diffuse plaque and saturate it; Within each eating into the plate enter acid, and other acids are formed from microbial metabolism.
Dissociation equilibrium of plaque acids • The acid is salt, and also in the liquid medium as well as the crystal starts to dissociate. hydrogen ions + acid anions The active part of an acid is the hydrogen ion, and its strength is dependent on the quantity thereof.
When in the solution around HA acid is dissociate , begins the active effect of hydrogen ions; The hydrogen ions pass into the enamel and move in competitive reaction with calcium.
The hydrogen ions move into contact with the hydroxyapatite and combined with the phosphate and hydroxide ions of the crystal– form a monohydrogen phosphate ion(НРО42+) and (Н2О). They quickly leave the crystal and move in solutionТе Са 10(РО 4) 6(ОН) 2 ←→ Са 2+ + 6РО 43- + ОН - ↓ Н+ НРО42+Н20 ↓ Н+ monohydrogen phosphate Н2РО 4- dihydrogen phosphate ion
Processes of de-and remineralization of enamel in the oral environment Enamel constantly washind from saliva. The concentration of Ca2 + and PO4 ions in the saliva varies - under normal conditions - 1,5 mmol / l. At neutral pH in the mouth the amount of Ca2 + and PO4 ions is sufficient to saturate the medium. These conditions provide balance in the process of de-and remineralization and no significant ion motion.
Processes of de-and remineralization of enamel in the oral environment By acidification of the medium saturation with inherent apatite ions decreased sharply Starts quickly extracting of ions from enamel for her saturation. Critical pH = 5,5 - direction of movement of the ions only in the direction from the enamel to the solution performed only under demineralization Performed only process of demineralization
Thelong-termexposureofteethtolowconcentrationsoffluoride (asfoundinfluoridatedwater) resultsinthegradualincorporationoffluorideintotheexistinghydroxyapatite (HAP) crystalstoformfluorhydroxyapatite (FHA), whichismoreresistanttoaciddamage. Ендогенна Ф профилактика
Conversely, a higherconcentrationoffluoride (asoccurswiththeuseoftopicalfluorideapplications, fluoridedentifrices, foams, andvarnishes, etc.) resultsintheformationofsurfaceglobulesof CaF2 (asseeninelectronmicroscopeimages). • Ifphosphatesandproteinsofthesalivacoattheseglobules, theglobulesbecomemoreinsoluble. Локална Ф профилактика