Download
1 / 45
460 likes | 708 Vues
Molecular Epidemiology of HIV. Francine E. McCutchan, PhD Global Molecular Epidemiology Program. Supported by the US Military HIV Research Program, the Division of AIDS, NIAID, NIH, and the European Commission. Status of the Global Epidemic. 40 million infections worldwide

E N D
Molecular Epidemiology of HIV Francine E. McCutchan, PhD Global Molecular Epidemiology Program Supported by the US Military HIV Research Program, the Division of AIDS, NIAID, NIH, and the European Commission
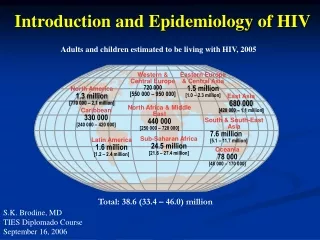
Status of the Global Epidemic • 40 million infections worldwide • More that 150 countries on 6 continents • Most infections are acquired heterosexually and affect men and women in equal numbers • A major cause of mortality in young adults • Substantial rates of perinatal transmission in much of the developing world • The epidemic continues essentially unabated in the absence of an effective vaccine
Worldwide Distribution of HIV Infections 1.4 million 610,000 1.0 million 1.1 million 540,000 440,000 7.1 million 25.4million 1.7 million 35,000 Source: UNAIDS Report on the Global Epidemic, 2004
Origins and Epidemic Spread • HIV-1 and HIV-2 • HIV-1 group M, N,O • HIV-1 Group M subtypes and recombinants • Different primates • Different introductions • Spread in human populations
HIV-1 and HIV-2 HIV-1 Group N, O, M HIV-1 Group M HIV-2 Group N HIV-1 Group O subtypes Group M recombinants The origins of HIV in Africa are reflected in its current distribution
Sources of Variation • HIV-1 is the most genetically variable of human pathogens • Rapid replication rate • High mutation rate • Recombination • HIV in the infected individual exists as a swarm of highly related but non-identical viral genomes termed a “quasispecies”
Rapid replication ~1010 virions per day High mutation rate ~1 substitution per genome per round Recombination ~7-30 crossovers per genome per round
HIV-1 Group M Subtypes and Recombinants • Nine Subtypes • Phylogenetically distinct across the genome • Inter-subtype Recombinants • At least 21 Circulating Recombinant Forms (CRF) • Numerous Unique Recombinant Forms (URF)
Phylogenetic Criteria for Classification: Subtype A J G 100 100 H 100 100 100 K 100 100 C 100 100 F D B 0.10
Phylogenetic Criteria for Classification: Subtype vs. Recombinant
Phylogenetic Criteria for Classification: CRF Chiang Mai B QuickTime™ and a Chaing Mai Graphics decompressor are needed to see this picture. D F C Bangkok H Rayong Bangkok A ‘ CRF01_AE Rayong CRF15_01B G J .10 gag gag pol env pol env GP120 GP41 GP120 GP41 100 90 80 Four Recombinant strains of identical structure recovered from widely separated locations in Thailand in 2003 established CRF15_01B 100 70 ‘ E ’ B 90 ‘ E ’ 60 50 80 40 70 30 ‘ ’ 60 ‘ ’ 20 50 10 40 0 30 20 10 0 CRF01_AE B CRF01_AE
Phylogenetic Criteria for Classification: URF URF A Kenya ACD KER2017 KER2021 AD MSA4071 AD AD KISII5003 AD KSM4015 KSM4017 AD KSM4028 AD AC KNH1097 AC MSA4080 AC KISII5011 AG KNH1043 CD MSA4077
Recombinant HIV-1 • Recombinant HIV are an important and particularly dynamic component of the global epidemic, and insight into their genesis and spread is of crucial importance for treatment and prevention • Genotyping of HIV strains is complicated by recombination, and requires suitable approaches • Complete sequencing of the genome of each strain provides an unequivocal classification • The database of complete genome sequences has grown exponentially in recent years
The HIV Sequence Database A B C D F, G, H, J, K Global prevalence High High High High Low Complete Genome Sequences 62 129 209 47 25 Subtype CRF01_AE CRF02_AE CRF03 through CRF16 High High Low 52 38 60 CRF AC, AD, CD, ACD Complex BF CRF01_AE/B Low Low Low Low 44 33 31 13 URF 743
Global Prevalence and Distribution • Subtype C accounts for almost 50% of HIV-1 infections worldwide • Globally prevalent strains include subtypes A, B, C, D, and CRF01_AE, CRF02_AG • Many regional epidemics contain a mixture of subtypes, while others are dominated by a single subtype or CRF • The regional epidemic patterns of HIV are varied, complex, and dynamic
The distribution of HIV-1’s subtypes and recombinants is as dynamic as its human host Be a virus, see the world…
Examples of a changing global epidemic • CRF01_AE a minor strain in Central Africa, but gained global importance as it entered Southeast Asia • Two new BC recombinant CRF circulate in China along different drug trafficking routes • A subtype A strain of low diversity, and a new CRF, CRF03_AB, emerged in former Soviet Republics after the dissolution of the Soviet Union destabilized the social milieu • CRF14_BG arose among IDU in Spain and Portugal in recent years • Subtype F, a rare strain in Central Africa, emerged in the form of BF recombinant strains, including a new CRF, in the Southern cone of South America
Kenya Uganda Tanzania The Genesis of Recombinant Strains URF A URF D A URF C A 30-40% of strains in mixed-subtype epidemics can be unique recombinants 120 complete genomes
Hypothesis • Some of the individuals who harbor URF are themselves co-infected with two or more HIV-1 strains • High risk, multiply exposed cohorts may exhibit a higher proportion of URF and dual infection compared to their lower-risk counterparts • The proportion of URF may increase over time in highly exposed cohorts due to ongoing re-infection
Approach • Develop tools for HIV-1 genotyping that are high throughput and capable of detection of both unique recombinant forms and dual infections • Establish cohorts exposed to a similar mixture of subtypes and recombinants in a given geographic region that represent various levels of HIV-1 incidence, prevalence, and risk • Perform genotyping cross sectionally at baseline and during longitudinal follow-up • Explore the viral dynamics and nature of the quasispecies in dual infections
Multi-Region Hybridization Assays (MHAs) • Fluorescent, subtype-specific probes spaced along the genome • Real-time PCR to provide automated, high throughput data collection and analysis • Validated against complete genome sequences for their ability to distinguish subtypes and recombinant forms • Capability to detect dual infections
A Family of MHAs for Regional Application Region East Africa West/Central Africa Southeast Asia South America Subtypes A, C, D, recombinants CRF02_AG, recombinants CRF01_AE, B, recombinants B, C, BF recombinants Assay MHAacd MHAcrf02 MHAbce* MHAbcf *Oral presentation (Kijak et.al.) in Molecular Epidemiology and Transmission session later this morning
Single infection Dual infection Stable quasispecies Fluctuating quasispecies Subtype Recombinant * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * * AAAA AAAA AAAA AAAA AAAA AAAA ACCCA AAAA AAAA ACCCA AAAA CCCC CCCC AAAA AAAA AAAA ACACACAC ACACACAC AAAA AAAA Assay Principle of the MHAacd for East Africa Visit 1 2 3 4
Comparative Epidemiology in East Africa Cohorts MHA Country Tanzania Tanzania Uganda Kenya Cohort HISIS CODE MER Kericho Population High risk females Urban and rural communities Rural communities Agricultural Plantation Genotypes (N) 238 487 329 366 1420
A URF URF URF A C D D Proportions of Recombinant HIV Using a cross sectional sample frame…. Urban High Risk Agricultural/Rural Rural/Urban URF 26.4% 29.5% 35.9% 50.8% MER KERICHO CODE HISIS A A URF C
Proportions of Dual Infections Using a cross sectional sample frame…. Urban High Risk Agricultural/Rural Rural/Urban MER KERICHO CODE HISIS URF 26.4% 29.5% 35.9% 50.8% Dual 16.4% 7.0% 7.1% 15.0%
These data are consistent with the hypothesis that some individuals become dual infected with more than one HIV-1 subtype, and that URF are the result They also suggest that both high and low risk cohorts are susceptible to dual infection, albeit to different degrees Increased dual infection Expansion of URF component Elevated risk
Longitudinal vs. Cross Sectional Sampling Mean 6.24 visits The HISIS high risk cohort was serially sampled every three months and genotyping was performed at each visit for 238 individuals ….. 100 90 80 70 60 N 50 40 30 20 10 0 1 to 3 4 to 6 7 to 9 10 to 12 Visits genotyped Cross sectional Longitudinal URF 50.8% 70.0% Dual 43.3% 16.4%
7.0 6.0 5.0 4.0 3.0 Fold Change 2.0 1.0 0.0 -1.0 -2.0 AC AD CD ACD A C D AC AD CD ACD Single Dual Changing Distribution of Subtypes and Recombinants during follow-up of the HISIS cohort
Kenya Uganda Tanzania Summary of Comparative Molecular Epidemiology in East African Cohorts • Identification of a significant fraction of both URF and dual infections in all cohorts studied • Association between higher multiple exposure risk and higher rates of dual infection • Association between dual infection and an increasing fraction of URF
Viral Dynamics in the Dual Infected Individual Possible outcomes of dual infection: • Persistence of two HIV-1 strains without detectable recombination • Virtual elimination of one of the original strains by selection • Generation of a new recombinant form that dominates the quasispecies, eclipsing the original strains • Continuous succession of new recombinant forms • Stable proportions of original strains and their recombinants over time • Changing proportions of original strains and their recombinants over time
Strategy for Assessment of Viral Dynamics gag nef vif vpu env pol vpr 1.36 KB 1.41 KB 1.44 KB • Amplify 1, 2 or 3 genome regions using multiple primer pairs for each region • Clone and sequence about 20 clones per region • Repeat for 2 to 5 visits per individual • Phylogenetic analysis of sequences to identify molecular forms, their relationships, proportions at each visit, and fluctuations over time
B D C V, VI, VII 100 100 A 100 I, II, III, IV 0.10 Molecular forms of gag in a dual infection One year follow-up, 66 clones… Form Structure Subtype A AC AC AC AC AC AC I II III IV V VI VII
III I IV I x V III V VI x I II I IV VII V I I II VI V I VII V Relationships of recombinant forms in a dual infection Probable original strains Derived recombinants VI
Persistence of many molecular forms and changing proportions over time…. I I V Number of clones V I V 12
The presence of multiple recombinant forms is a consistent feature of dual infections Case 123 442 507 529 551 Analysis Molecular Forms gag 7 3 3 4 3 gp120 n.d. n.d. 8 n.d. 1 gp41 5 3 4 1 n.d. Visits 4 2 5 4 3 Genes 2 2 3 2 2 Clones 152 95 298 185 107
Temporal Fluctuation of the Viral Quasispecies 123 gag gp41 442 gag gp41 507 gag gp120 gp41 529 gag gp41 551 gag p120 0 3 6 9 12 15-21 Sample Interval (months)
Viral Dynamics in Dual Infected Individuals • Persistence of two HIV-1 strains without detectable recombination • Virtual elimination of one of the original strains by selection • Generation of a new recombinant form that dominates the quasispecies, eclipsing the original strains • Continuous succession of new recombinant forms • Stable proportions of original strains and their recombinants over time • Changing proportions of original strains and their recombinants over time X X X X X X √
Implications of Dual Infection - Epidemiology • Detection of dual infections is an essential element of HIV-1 genotyping • Each dual infected individual could be the source of a series of different recombinants during the course of infection, amplifying the fraction of URF in the population • A dual infected individual could transmit more than one strain simultaneously, thereby increasing the dual infected population directly • Effective interventions in populations susceptible to dual infection may limit the genetic complexity of HIV strains, both URF and the eventual emergence of CRF
Implications of Dual Infection - Vaccines Why does HIV infection sometimes fail to protect against re-infection? • Damage to the human immune system at the time of initial HIV-1 infection • Failure of cross-protective immunity resulting from the high genetic diversity of HIV-1 • Some combination of the above
Implications of Dual Infection -Pathogenesis • By 2004, studies in the US and in Africa had associated dual infection with increased viral load and/or rapid disease progression The Lancet, 2004 Gottlieb et.al. JID, 2004 Grobler et.al. AIDS 2004 Manigart et.al. • Yet, it is unclear which is cause and effect • More severe initial damage to the immune system may predispose to rapid progression and increase susceptibility to re-infection • Dual infection could generate a more diverse and difficult to control viral quasispecies, which could accelerate disease progression
Implications of Dual Infection - Transmission • Higher plasma viral loads associated with increased transmission • Dual infection associated with higher plasma viral loads It is possible that the very individuals who become dually infected also develop a higher plasma viral load that renders them particularly efficient at transmission of the recombinant forms that arise within them
Conclusion By specifically addressing the factors that foster dual infection and the generation and transmission of recombinant HIV-1, benefit may accrue to the individual, in terms of preventing a more rapid disease progression, and to society, by limiting the complexity of strains that must eventually be controlled by treatments and vaccines. In the future, prevention of re-infection of those already infected with HIV-1 may become an important element in the overall strategy to gain control of the global epidemic
Thanks to the many collaborators and to the participants in cohort studies in Africa Makerere University and Uganda Virus Research Institute Nelson Sewankambo David Serwadda Mbeya Medical Research Programme US Military HIV Research Program Michael Hoelscher Martina Gerhardt Leonard Maboko Donan Mmbando Eluter Samky Oliver Hoffmann Steffan Geis Miguel Arroyo Sucheep Piyasirisilp Sodsai Tovanabutra Gustavo Kijak Eric Sanders-Buell Merlin Robb Deborah Birx Colombia University and Johns Hopkins University Maria Wawer Ron Gray US Army Medical Command Kenya and Kenya Medical Research Institute Ginamarie Foglia Monique Wasunna Sam Martin Wilfred Langat