Download
1 / 25
250 likes | 400 Vues
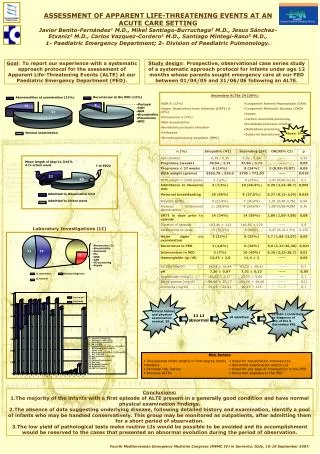
ACUTE LIFE THREATENING EVENT. SUDDEN UNEXEPECTED DEATH IN INFANCY.

E N D
SUDDEN UNEXEPECTED DEATH IN INFANCY I Injury * Accidental Infection *Sudden infant death Syndrome *Sever pneumonia *Deliberate Congental Anomaly *Sepsis * Subendocardiac *Gasteroenteritis *Fibroelastosis *Long QT Syndrome *Cardiac Anomaly *Pulmonary Anomaly *Neurological Anomaly
case FT baby 6days old, producte of home vaginal delivary with PROM>24hr ,he had fever&vomting,poor sucking laste 3days.O/E ;Lethargic,febrile(38C) NN reflex weak
Neonatal sepsis It is the systemic inflammtoryrespones to an infection process. The most commen cause; GBS , E-Coli ,L-monocytogenus Other causes are ;(non-bactrial) Viral , protozal , fungal
Etiologic Agents of Neonatal Pneumonia According to Timing of Acquisition
Risk factors Maternal Intrapartum fever(>38) PRM(>18hr) Chorioaminionits PT labor(<37wk) Neonatal Male sex PT& LBW Cong—anomalies Immunity defect Galactosemia(E-Coli)
Clinical manifestation General; Fever.temperature instability Poor feeding GIT; Diarreh,Vomiting Abd-distention Respiratory; Apnea,RDS Renal; oliguria CNS; Irritability,lethargy,seizers High pitch cry,hypotonia, Full fontanel, CVS; Pallor,mottling,HR( ) hypotention, Hematology; Jaundies, pallor,petechia,purpura Bleeding
Diagnosis; sepsis workup; *Culture; Blood—CSF—Urine *CBC; WBC(<5000), ANC<1750, I : T>0,2 *CRP *G.stain;CSF,Urine;Infected side *Chest Xry
Treatment Once the pathogen has been identified & antibiotic sensitivities determined, the most appropriate drug or drugs should be selected. For most gram-negative enteric bacteria, Ampicillin & an Aminoglycoside or a 3rd-generation cephalosporin (cefotaxime or ceftazidime) should be used. Enterococci should be treated with both a penicillin (Ampicillin or piperacillin) & an aminoglycoside because the synergy of both drugs is needed. Ampicillin alone is adequate for L. monocytogenes, and penicillin suffices for GBS. Clindamycin or metronidazole is appropriate for anaerobic infections
Treatment Is determined by pattern of disease and the organisms that are common for the age of infant& the flora of the nursery. Duration of Rx; meningits(14—21days) Pneumonia(7—10)
DDX CVS; CHD.myocaditis,PPHN GIT; Necrotizing enterocolitis spontanousGITperfora-tion Hematology; Nnpurpuric fulminans Sever anemia Immune mediated neutropenia&thromboc-ytopenia Respiratory; RDS,lung hypoplasia TEOF,aspiratin pneumonia, Metabolic; Hypoglysemia Galactosemia CNS; HIE.Infant botulism ICH
prognosis&complication The risk factors for death or for moderate or sever disability include; *Duration of seizeres >72hrs *Coma *Necessity for the use of inotropic agents *Lukopenia
The acronym TORCH refers to toxoplasmosis, other agents (syphilis, etc.), rubella, CMV, and HSV. the TORCH battery of serologic tests has a poor diagnostic yield, and appropriate specific diagnostic studies should be selected for each etiologic agent under consideration. CMV & HSV require culture or (PCR) methods, whereas syphilis, toxoplasmosis, & rubella are diagnosed by specific serologic methods
prevention Aggressive management of suspected maternal chorioamnionitis with antibiotic therapy during labor,along with rapid delivaryof the infant,reduces the risk of early Nnsepsis. Intrapartum chemoprophylaxsis reduced the vertical transmission of GBS.
Sudden infant death syndrome That is unexpected by history and unexplained by a thorough postmortem examination ,which includes a complete autopsy,investigation of the scene of death, and review of medical history.
Risk factors Maternal; Smoking,Drugs Nutritional deficiency Decreased age,education Single marital status IGR,increas parity Low socioeconomic status Infant; Age(2-4mo),PT,Male Pron sleep position Growth failure Recent(febrile) illness Soft bedding
NEONATAL SEPSIS Objectives; *Definition Factors ; Risk * Mternal &neonatal * Types & clinical manifestation l Diagnosis * Treatment * Prognosis * Prevention * *DD