Download

1 / 59
630 likes | 1.32k Vues
Gynecomastia. Question. 24 year-old male presents to PCP for painless enlargement of breasts for past six months Gradual onset without discharge or pain No past medical history, medications, or supplements Social ETOH use – less than 5 drinks per week Exam: BMI: 31

E N D
Question • 24 year-old male presents to PCP for painless enlargement of breasts for past six months • Gradual onset without discharge or pain • No past medical history, medications, or supplements • Social ETOH use – less than 5 drinks per week • Exam: • BMI: 31 • Breast – bilateral retro-areolar rubbery mass • Testicular – No masses, tenderness; normal size • Evaluation: • LH – 4.8 mIU/ml (NML 1.5-9.3 mIU/ml) • Testosterone – 482 ng/dl (NML 241/827 ng/dl) • TSH - 0.52 mIU/ml (NML 0.4-5.5 mIU/ml)
What is the next step? • Observation – this will likely regress • Referral for elective surgery – patient has cosmetic concerns regarding breasts • Trial of tamoxifen for six months • Encourage weight loss and ETOH avoidance with follow-up • Work-up is not complete – continue evaluation
Take Home Points • Gynecomastia may be a transient complaint, or the only manifestation of a fatal disease • Gynecomastia requires a thorough investigation for cause; including hormonal evaluation if indicated • Treatment of gynecomastia is cause specific
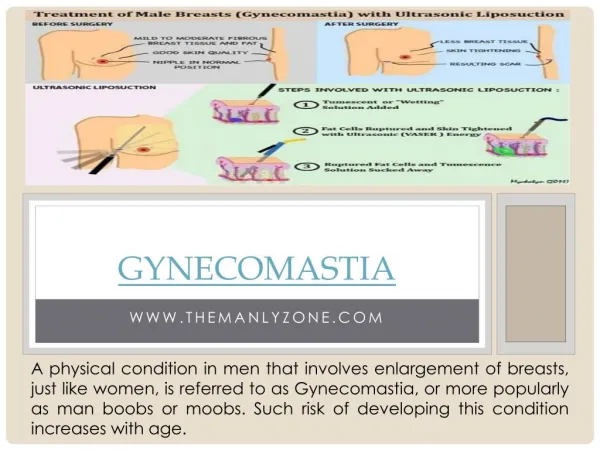
Definition • Clinical: • Rubbery or firm mass extending concentrically from the nipple • Pathologic: • Benign proliferation of the glandular tissue of the male breast • Pseudo-gynecomastia • Fat deposition without glandular proliferation
Histology • Initial: 1) Ductal epithelial hyperplasia 2) Proliferation of periductal inflammatory cells 3) Periductal fibroblastic proliferation. • Late (after >12 month): 1) Increased number of ducts with dilatation 2) No epithelial cell proliferation 3) Increased fibrosis Normal male breast Early gynecomastia www.uptodate.com
Epidemiology • Common at birth • Found in up to 60 - 90% of male infants • Second peak in puberty • Estimated at 4-69% of males • Most common ages 11-12 (Tanner 3) • Uncommon after age 17 • Highest peak ages > 50 • Estimated 24-65% of men affected Braunstein G. N Engl J Med 1993;328:490-495
Prevalence of gynecomastia from multiple population studies Braunstein. Gynecomastia. In: Diseases of the Breast. Harris, Lippincott-Raven, Philadelphia 1996. p. 54.
Pathophysiology Braunstein G. N Engl J Med 1993;328:490-495
Etiologies • Persistent pubertal gynecomastia 25% • Medications 10 - 25% • Idiopathic 25% • Cirrhosis or malnutrition 8% • Hypogonadism: • Hypergonadotropic 8 % • Hypogonadotropic 2 % • Testicular tumors 3% • Hyperthyroidism 1.5% • Chronic renal insufficiency 1% Braunstein, Glenn.“Gynecomastia”. NEJM 1993;328:490-95
Persistent Pubertal Gynecomastia • Usually occurs age 11-12 (Tanner 3) • Initial estradiol surge at puberty • Followed by testosterone surge • Persists up to two years in 25% Hands, L. Gynaecomastia. Br. J. Surg. 1991, 78:907-911
Etiologies • Persistent pubertal gynecomastia 25% • Medications 10 - 25% • Idiopathic 25% • Cirrhosis or malnutrition 8% • Hypogonadism: • Hypergonadotropic 8 % • Hypogonadotropic 2 % • Testicular tumors 3% • Hyperthyroidism 1.5% • Chronic renal insufficiency 1% Braunstein, Glenn.“Gynecomastia”. NEJM 1993;328:490-95
Medications Braunstein G. N Engl J Med 1993;328:490-495
Spironolactone • Symptoms in almost every male at doses of 100 mg/day • Small study of six patients on spironolactone with gynecomastia compared to control patients • Spironolactone patients had significantly lower testosterone and higher estradiol (p<0.01) • Androgen receptor antagonist • Increased peripheral aromatization to estradiol • Decreased testosterone production Rose, L. Ann Intern Med 1977;87:398-403
Spironolactone • Randomized Aldactone Evaluation Study (RALES) • Evaluate spironolactone in heart failure • Double-blind, placebo controlled with 1663 patients included in study • Spironolactone or placebo at 25 – 50 mg daily • Trial stopped early due to significant reduction in cardiovascular mortality • Gynecomastia • Treatment group - 9% (p<0.001) • Placebo group - 1% • In a second study, epleronone, a selective aldosterone antagonist, had equal incidence of gynecomastia as placebo in over 6500 patients Pitt, B et. Al. NEJM 1999;341:709-17; NEJM 2003;348:1309-21
Anti-Ulcer Medications • Many case reports of gynecomastia related to anti-histamine and proton pump inhibitor medications • Open cohort study from UK – 1989-92 • Evaluated 81,535 men aged 25-84 given prescription for cimetidine, omeprazole, or ranitidine • Omeprazole and ranitidine had no increased risk of gynecomastia • Cimetidine had significant increased risk for gynecomastia (RR 7.2) • Noted verapamil RR 9.7 and spironolactone RR 9.3 Rodriquez, LA. “Risk of gynaecomastia associated with cimetidine, opeprazole, and other antiulcer drugs”. BMJ 1994;308:503-6
Anti-Androgen Medications • Flutamide, bicalutamide, nilutamide • Used commonly in prostate cancer to suppress androgen stimulation of cancer • Bind to androgen receptors to block testosterone and DHT response • Excess testosterone aromatized to estradiol • Finasteride • 5-alpha reductase inhibitor • Blocks conversion of testosterone to DHT
Drugs • Other well described association: • ETOH • Inhibition of H-P-T axis as well as direct testicular toxicity • Marijuana • Androgen receptor antagonist • Tree oils and lotions • Any estrogen containing creams • HAART • More commonly pseudo-gynecomastia • Lipodystrophy also possible Warren, S. “Lipodystrophy” NEJM 2005;352:62
Etiologies • Persistent pubertal gynecomastia 25% • Medications 10 - 25% • Idiopathic 25% • Cirrhosis or malnutrition 8% • Hypogonadism: • Hypergonadotropic 8 % • Hypogonadotropic 2 % • Testicular tumors 3% • Hyperthyroidism 1.5% • Chronic renal insufficiency 1% Braunstein, Glenn.“Gynecomastia”. NEJM 1993;328:490-95
Idiopathic/Obesity/Normal Aging • Androgen Insensitivity • Aromatase excess • Due to excess adipose tissue • Hereditary aromatase excess
Idiopathic/Obesity/Normal Aging Braunstein, Glenn.“Aromatase and Gynecomastia”. Endocrine-Related Cancer 1999;6:315-24
Etiologies • Persistent pubertal gynecomastia 25% • Medications 10 - 25% • Idiopathic 25% • Cirrhosis or malnutrition 8% • Hypogonadism: • Hypergonadotropic 8 % • Hypogonadotropic 2 % • Testicular tumors 3% • Hyperthyroidism 1.5% • Chronic renal insufficiency 1% Braunstein, Glenn.“Gynecomastia”. NEJM 1993;328:490-95
Cirrhosis/Starvation • Several mechanisms: • Decreased clearance of androgens leading to increased conversion to estrogen • Increased sex hormone binding globulin (SHBG) decreasing free testosterone • Decreased testosterone production
Etiologies • Persistent pubertal gynecomastia 25% • Medications 10 - 25% • Idiopathic 25% • Cirrhosis or malnutrition 8% • Hypogonadism: • Hypergonadotropic 8 % • Hypogonadotropic 2 % • Testicular tumors 3% • Hyperthyroidism 1.5% • Chronic renal insufficiency 1% Braunstein, Glenn.“Gynecomastia”. NEJM 1993;328:490-95
Hypergonadotropic Hypogonadism • Predominance of adrenal androgens with peripheral conversion to estradiol • Congenital: • Klinefelter’s Syndrome • Cryptorchidism • Myotonic dystrophy and other rare androgen receptor disorders • Acquired: • Drugs • Viral or traumatic injury • HIV and mumps • Radiation injury • Chronic illness • Hemochromatosis • Autoimmune disease Bagatell, C. Androgens in Men – Uses and Abuses. NEJM 1996;334:707-14
Hypogonadotropic Hypogonadism • Predominance of adrenal androgens • Testicular estradiol production may persist
Etiologies • Persistent pubertal gynecomastia 25% • Medications 10 - 25% • Idiopathic 25% • Cirrhosis or malnutrition 8% • Hypogonadism: • Hypergonadotropic 8 % • Hypogonadotropic 2 % • Testicular tumors 3% • Hyperthyroidism 1.5% • Chronic renal insufficiency 1% Braunstein, Glenn.“Gynecomastia”. NEJM 1993;328:490-95
Testicular Neoplasm • Germ cell cancers (95% of testicular cancer) are associated with gynecomastia in 2.5-6% • Most common with elevated hCG from choriocarcinoma • hCG stimulates aromatase in Leydig cells • Poor prognostic indicator – 50% mortality rate in small case series of cases • Incidence of gynecomastia is 20-30% with Leydig cell cancers (2% of all testicular cancers) • Leydig cells produce high levels of estradiol • Commonly occurs after treatment of testicular cancer due to hypergonadotropic hypogonadism • Does not change prognosis if symptoms occur after treatment Tseng, A. “Gynecomastia in testicular cancer patients. Prognostic and therapeutic implications.” Cancer 1985; 56:2534.
Etiologies • Persistent pubertal gynecomastia 25% • Medications 10 - 25% • Idiopathic 25% • Cirrhosis or malnutrition 8% • Hypogonadism: • Hypergonadotropic 8 % • Hypogonadotropic 2 % • Testicular tumors 3% • Hyperthyroidism 1.5% • Chronic renal insufficiency 1% Braunstein, Glenn.“Gynecomastia”. NEJM 1993;328:490-95
Thyrotoxicosis • Multiple pathways: • Increased Sex Hormone Binding Globulin (SHBG) • Increased androstenedione production rates • Increased peripheral aromatization of testosterone to estradiol Pearlman, G. The Endocrinologist 2006;16:109-15
Etiologies • Persistent pubertal gynecomastia 25% • Medications 10 - 25% • Idiopathic 25% • Cirrhosis or malnutrition 8% • Hypogonadism: • Hypergonadotropic 8 % • Hypogonadotropic 2 % • Testicular tumors 3% • Hyperthyroidism 1.5% • Chronic renal insufficiency 1% Braunstein, Glenn.“Gynecomastia”. NEJM 1993;328:490-95
Renal Failure • Similar mechanism to starvation • Decreased testicular function preceding dialysis • Increased hormone production after initiating dialysis with increased estrogens first
Review:Etiologies of Gynecomastia www.cbsnews.com Braunstein G. N Engl J Med 1993;328:490-495
Differential Diagnosis • Pseudo-gynecomastia • Breast cancer • Lipoma or cyst Hannekin, S. Ann Int Med 2004;140:497-98
Evaluation • History and Physical Exam Including: • Onset and duration of symptoms • Detailed medication history • Evaluation for evidence of other systemic disease • Physical exam focus: • Body habitus, body mass index • Bilateral breast exam • Testicular exam: Size, masses • Hair distribution • Thyroid exam
Evaluation • Red flags: • New onset • No risk factors or common medications • Young, post-puberty • Painful • Hard nodule • Nipple discharge
Hormonal Evaluation • Indicated if no obvious cause for symptoms on history and physical • Laboratory evaluation: • LH • hCG • Testosterone (including free fraction) • Estradiol • TSH
Elevated hCG = cancer Low testosterone = hypogonadism High estradiol = cancer or aromatase Braunstein G. N Engl J Med 1993;328:490-495
Radiographic Evaluation • Consider testicular ultrasound • Mammogram to evaluate for cancer: • Klinefelter’s Syndrome • Family history of male breast cancer • Suspicious mass • Ultrasound effective to diagnose pseudo-gynecomastia
Mammography • In experienced centers: • Gynecomastia can be diagnosed • Suspicious nodular findings must be evaluated with biopsy • Overlap between malignant and benign limit utility Appelbaum, AH. Scientific Exhibit 1999;19:599-68
Treatment • Cause specific: • Stop offending medications • Weight loss • Alcohol cessation • Treatment of underlying disorder • Most idiopathic cases will resolve or regress within six months
Treatment • Medical therapy • No FDA approved treatment currently • Testosterone therapy if indicated for hypogonadism • Increased conversion to estradiol may worsen symptoms • Anti-estrogen therapy: Tamoxifen or clomiphene • Aromatase inhibitor therapy: anastrozole