ST ELEVATION
ST ELEVATION. Jason Mitchell, PGY2 July 15, 2010. Context. CP and ST Elevation common ED presentation Correct ECG interpretation impacts management decisions and patient outcome Certain patients with CP and ST elevation require rapid intervention via thombolysis or PCI

ST ELEVATION
E N D
Presentation Transcript
ST ELEVATION Jason Mitchell, PGY2 July 15, 2010
Context • CP and ST Elevation common ED presentation • Correct ECG interpretation impacts management decisions and patient outcome • Certain patients with CP and ST elevation require rapid intervention via thombolysis or PCI • Misdiagnosis potentially harmful
Context • 1996 ACC/AHA Class I Recommendation for Thrombolysis • “ST elevation greater than 0.1 mV in two or more contiguous leads.”1 1 Ryan TJ, Anderson JL, Antman EM, et al. ACC/AHA guidelines for the management of patients with acute myocardial infarction. A report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines (Committee on Management of Acute Myocardial Infarction). .J Am CollCardiol. 1996 Nov 1;28(5):1328-428
Context • Disorders with ST Elevation Meeting ACC/AHA Thrombolysis Guideline
Context • 2000 ACEP Qualifier • “ST-segment elevations greater than 0.1 mV in 2 or more contiguous leads that are not characteristic of early repolarizationor pericarditis, nor of a repolarization abnormality from LVH or BBB in patients with clinical presentation suggestive of AMI.”2 2 Critical issues in the evaluation and management of adult patients presenting with suspected acute myocardial infarction or unstable angina. Ann Emerg Med 2000;35:521-525
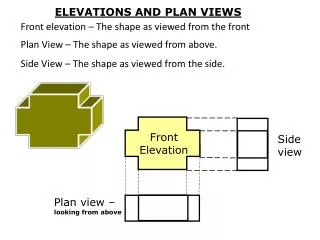
ST Morphology • Concave Up vs. Concave Down
ST Morphology • Concave Up vs. Concave Down
ST Segment Elevation • Differentiating STEMI from other ST Elevation Syndromes • Dynamic ECG changes • Reciprocal Changes
STEMI Territories • Localizations
Context • 2000 ACEP Qualifier • “ST-segment elevations greater than 0.1 mV in 2 or more contiguous leads that are not characteristic of early repolarizationor pericarditis, nor of a repolarization abnormality from LVH or BBB in patients with clinical presentation suggestive of AMI.”2 2 Critical issues in the evaluation and management of adult patients presenting with suspected acute myocardial infarction or unstable angina. Ann Emerg Med 2000;35:521-525
Early Repolarization • Normal variant • Males > Females • ECG Findings: • Diffuse, Concave up ST Elevation 2-5mm (Usually precordial) • Notched J-Point • Prominent T-Waves • Temporal stability
Early Repolarization • “Benign” Early Repolarization • Increased prevalence of early repolarization in idiopathic VF • Most pronounced with inferior J-Point elevation • Increased risk of cardiac death (ie – sudden arrythmia) • J-Point 1mm: RR 1.28, 95% CI 1.05 – 1.59 • J-Point 2mm: RR 2.98, 95% CI 1.85 – 4.923 • Isolated BER in limbs leads should prompt ACS investigations 3Tikkanen JT, Anttonen O, Junttila MJ, et al. Long-term outcome associated with early repolarization on electrocardiography. N Engl J Med. 2009 Dec 24;361(26):2529-37.
Pericarditis • Diffuse ST Elevation • Diffuse PR Depression • Caveat: aVR • ST Depression, PR Elevation
Pericarditis • Stages – All 4 Present in ~50% of patients • I – ST Elevation, concordant T-Waves, PR Depression • II – ST segments return to baseline, T-Waves flatten • III – T-Wave inversion • IV – T-Wave resolution
Pericarditis • Differentiation from STEMI • Concave Up ST segments • ST elevation beyond contiguous leads • No simultaneous T-Wave inversion • Reciprocal changes absent • Serial ECGs not consistent with STEMI patterns • No Q-Wave development
Pericarditis vs. BER • Differentiation of Pericarditis from BER • V6 ST/T Ratio • Pericarditis > 0.25 • BER < 0.25
LVH • Tall R waves lateral leads • Deep S waves anterior precordial leads • Concave Up ST elevation, typically V1-V3 • LAD
LBBB • Wide QRS • Large, positive R wave without q or s waves in I, aVL, V6 • Notched ‘M Shaped’ R wave V5, V6 • Normal or leftward axis • ST depression and T wave inversion in leftward leads • ST elevation and upright T waves in right precordial leads
LBBB • 7% of MI4 • Significantly less likely to receive ASA • Increased in-hospital mortality 4 Go AS, Barron HV, Rundle AC, et al. Bundle-branch block and in-hospital mortality in acute myocardial infarction. National Registry of Myocardial Infarction. Ann Intern Med 1998 Nov 1;129(9):690-7.
LBBB • Sgarbossa Criteria5 • Score ≥ 3 • 98% specific • 20% sensitive6 5Sgarbossa EB, Pinski SL, Barbagelata A, et al. Electrocardiographic diagnosis of evolving acute myocardial infarction in the presence of left bundle-branch block. GUSTO-1 (Global Utilization of Streptokinase and Tissue Plasminogen Activator for Occluded Coronary Arteries) Investigators. N Engl J Med 1996 Feb 22;334(8):481-7. 6Tabas JA, Rodriguez RM, Seligman HK, et al. Electrocardiographic criteria for detecting acute myocardial infarction in patients with left bundle branch block: a meta-analysis. Ann Emerg Med. 2008 Oct;52(4):329-336.e1.
LBBB • ECG Evolution • Anterolateral MI • New S Waves in Leftward Leads • I, aVL, V6 • Anteroseptal MI • Lateral q waves • I, aVL, V5-V6
RBBB? • Can present with ST elevation • No impact on initial QRS vector • Q waves are not changed
Conclusion • Evaluate ECG in relation to clinical presentation • ST morphology • Dynamic ECG changes, serial ECGs • Look for reciprocal changes
Practice • Inferior MI • V1 Elevation: RV Infarct • ST Elevation III > ST Elevation II: RCA Occlusion
Practice • Hyperacute Anterior MI • Note Mobitz II Conduction Block • Malfunctioning His-Pukinje system • Suggests anterior occlusion • Ie - LAD occlusion • Mobitz I Conduction Block • Malfunctioning AV node • Suggests ‘dominant’ coronary occlusion • RCA or Circumflex
Practice • PosteriorMI • Note ‘q’ waves in anterior leads
Practice • WPW
Practice • LBBB Concerning for MI
Practice • Anterior MI