Clinical PATHOLOGY
Clinical PATHOLOGY. BY: DR (MRS) B.J.THANENTRHIRAN(MBBS). Pathology is the study (logos) of suffering (pathos). Pathology address following components of disease. Cause / Etiology Incidences Mechanisms of development ( pathogenesis )

Clinical PATHOLOGY
E N D
Presentation Transcript
Clinical PATHOLOGY BY: DR (MRS) B.J.THANENTRHIRAN(MBBS)
Pathology is the study (logos) of suffering (pathos). • Pathology address following components of disease. • Cause / Etiology • Incidences • Mechanisms of development (pathogenesis) • Structural alterations of cells (morphologic changes) • Consequences of changes (clinical manifestations)
Pathology Anatomic pathology Clinical pathology
Anatomic pathology is concerned with the diagnosis of disease based on the gross, microscopic, chemical, immunologic and molecular examination of organs, tissues, and whole bodies (autopsy).
Clinical pathology is concerned with the diagnosis of disease based on the laboratory analysis of • body fluids • and tissues • using the tools of • Chemistry • Microbiology • Hematology • and Molecular pathology
Subsections • Anatomic pathology • Cytopathology • Histopathology • Surgical pathology • Clinical pathology • Hematology • Chemical pathology • Microbiology • Immunology • Urinalysis • Blood bank
Cytopathologyis a branch of pathology that studies and diagnoses diseases on the cellular level. • Histopathology refers to the microscopic examination of tissue in order to study the manifestations of disease. • Surgical pathology involves the gross and microscopic examination of surgical specimens and biopsies.
Cytopathology / cytology Cell collection • Exfoliative cytology • Cells from spontaneous exfoliation • Cells from mechanical exfoliation(scraping/brushing) • Intervention cytology • Intervening into the body for sample collection • FNAC – Fine Needle Aspiration Cytology
Indications for cytopathology • Diagnosis of malignancy and its type • Diagnosis of premalignant diseases • Detection of inflammation and certain types of pathogenic agents • Study of the hormonal patterns and evaluation of the gonadal hormonal activity.
Follow-up and monitoring of response to chemotherapy and irradiation. • The identification of sex chromosome. (Barr bodies) • Tumor markers study on cytological specimens
Following parameters are seen in the cellular sampling • Nucleus • Nucleolus • cytoplasm • In addition following pathologies can be seen. • Microbial infections • Reactive changes • Immune reactions • Cell aging • Amyloidosis • Autoimmune diseases
Cytology specimens • Fluids • Effusion into body cavities (pleural, peritoneal, pericardial) • Cyst aspirates • CSF • Urine • Sputum
Wash specimens – bronchial, bladder • Brush cytology – bronchial, cervical, gastro intestinal. • Pap smears • Bone marrow aspiration • Fine needle aspiration.
Advantages of cytology • Provides a rapid, inexpensive & simple diagnosis. • Little tissue injury. • Frequent sampling • Evaluation of progression to treatment / recurrence • Better accepted by the patient & clinician • Sample cells from wider surface than a biopsy
Cells can be obtained by inaccessible / difficult to access areas • Determination of hormonal states • Minimum distortion of cells • Smears permit better evaluation of the nature of inflammations and infections.
Limitations of cytology • Cytologic diagnosis is not always final. Must be confirmed by histology. • Diagnosis is based upon the study of minute cellular details. • Tissue pattern cannot be appreciated • Interrelation & arrangement of the cells to the supporting stroma cannot be established. • Location of lesion cannot be pin pointed (except in FNAC)
Size of the lesion cannot be estimated. • Error / misinterpretation may occur.
Fine Needle Aspiration Cytology (FNAC) • Used to investigate superficial lumps or masses. • Lung, intra-abdominal and retroperitoneal samples can be taken with the help of radiologic imaging (CT, ultrasound) • Sampling is done for diagnostic purposes and to asses the effect of treatment.
Advantages of FNAC • Easy, reliable, cost effective • Out patient procedure • Minor surgical procedure, No risk of anesthesia • Safer than open surgical biopsies • Easily repeatable • Less complications • Patient can go back to normal activities soon • Can get results rapidly
Disadvantages of FNAC • False negative results (some lesion do not exfoliate cells well, needle may miss the site of the lesion, timid collection, inadequate negative pressure). • Definitive diagnosis is difficult.
Complications of FNAC • Needle trauma • Needle track seeding - testicular tm, chondrosar • Hematoma • Pain
Preparations before the procedure • No use of aspirin or non-steroidal anti-inflammatory medications (e.g. ibuprofen, naproxen) for one week before the procedure • No food intake a few hours before the procedure • Routine blood tests (including clotting profile) must be completed two weeks before the biopsy
Suspension of blood anticoagulant medications • Antibiotic prophylaxis may be instituted. • Check vital signs before the procedure • IV line if necessary.
Equipments needed for FNAC procedure • Syringes • Standard disposable plastic syringes of 10ml are used. • Syringe should be of good quality and should produce good negative pressure. • Needles • Standard disposable 22-24 gauge 1-1½-inch needles are used for plain FNAC.
Slides • Plain glass slides of good quality are used. Slides should be clean, dry, transparent and grease free. • An important procedure is slide labeling at the time of sampling. • Fixatives • These are applied to the smears as a spray or by immersion of the slide into a liquid. • The most commonly used is 95 % Ethanol. • This inexpensive readily available liquid provides excellent cytological details. • Fixative is kept ready in Coplin jars. • Container
Other supplies • Test tubes, pencil for marking, alcohol, swabs for skin, watch glass, saline, adhesive dressing, gloves etc. are needed. • All the materials required are assembled in advance before starting the procedure. • This is extremely important as delay in fixation can make interpretation of smears difficult.
Steps to be followed before performing the aspiration • Relevant history and clinical details, radiological findings, provisional diagnosis etc. must be entered in the requisition form. Site of FNA must be clearly stated. • Lesion to be aspirated is palpated and its suitability for aspiration assessed. The appropriate needle is selected accordingly.
The procedure must be clearly explained to the patient and consent and co-operation ensured. Patient may be anxious which needs to be allayed. Ignoring this simple but crucial step can result in failure. • Before starting the procedure, ensure that all the required equipment, instruments and supplies are available. • All universal precautions should be followed during the procedure.
Steps to be followed during the aspiration • Position the patient. • Sterilize the skin above the area to be biopsied with antiseptics. • May use local anesthesia but often not necessary. • Locating the mass by palpation by non dominant hand.
Aspirates should be obtained using preferably a 23 gauge, 1 ½ inch disposable needle mounted on a 10 ml plastic syringe, held by the dominant hand. • The needle should be gently introduced through the skin passing to the level of the dominant mass. • Having confirmed the position of the needle within the mass, negative pressure should be created within the syringe by pulling back the plunger. • The needle should move back and forth through the mass, in different rotational directions.
Suction should be maintained throughout the process by outward. • All suction should be released before removing the needle from the mass. • Then the needle should be withdrawn gently from the mass. • To limit hematoma formation from the site of the puncture, firm pressure should be applied with a piece of cotton for two minutes.
Preservation and processing of Smears • Smears are prepared and fixed according to the requirements of the stain to be used. • Air-drying followed by hematological stains. • Alcohol fixation followed by Papanicolaou (pap) or hematoxylin and eosin (H&E) staining.
Preparation and fixation for pap/ H&E staining • Immediately after withdrawing, detach the needle, draw air into the syringe, reattach the needle and express the material in the needle onto a slide. • Needle tip is brought into light contact with the slide and the aspirate is carefully expressed without spraying into the air, which can cause air-drying and also can form aerosols, which are potentially infectious. • Aspirates are smeared immediately using another slide or cover slip or with the needle itself and dropped into the fixative.
The cells must be delicately and thinly smeared with minimal distortion and fixed according to the stain to be used. • Spreading the cells too thinly as well as preparing too many smears is an error because of cellular distortion or dilution. Thus the smears must be of adequate thickness.
Unsatisfactory smears can be due to non representative / inadequate samples or due to poor quality of preparation (thick smears, extreme admixture with blood, delayed fixation, over staining etc)
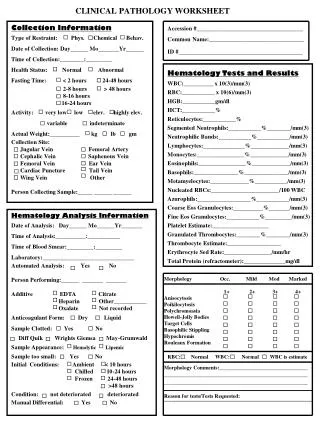
Quality control Measures • In addition to details of technique (procedure, preparation, quality of materials used) and clinical correlation; other routine quality control practices regarding specimen reception (checking patient details, identification of slides, number of slides from each patient, labeling the slides), preparation and maintenance of stains, staining procedure, mounting, record keeping etc. are needed for optimal quality of diagnosis.