
Sleep Apnea
E N D
Presentation Transcript
Sleep Apnea Everything You Never Wanted to Know About… By: John J. Beneck MSPA, PA-C
Case 1 • 35 year old male with loud snoring. Spouse states she can’t sleep in the same room with him.
Case 2 • 46 year old obese male in for annual CPE observed by you to appear sleepy during the medical interview.
Case 3 • In Hospital: Call at 0025 from RN that 42 year old female diabetic in with lower extremity cellulitis has oxygen saturation in the low 80s when checking vital signs. Awoke when stimulated and SaO2 improved.
Objectives • Understand OSAH and CSAS in terms of the following: • Definition • Epidemiology • Pt. Presentation • Dx • Prevention • Tx • Prognosis
CO2 – Carbon dioxide CPAP – Continuous positive airway pressure CPE – Comprehensive Physical Exam CSAS – Central sleep apnea syndrome CV – Cardiovascular D/t – due to Dx – Diagnosis Dz - Disease EEG – Electroencephalogram HF – Heart failure HTN – Hypertension LVEF – Left ventricular ejection fraction MVC – Motor vehicle crash N-CPAP – Nasal CPAP O2 - Oxygen OSAH – Obstructive sleep apnea hypopnea syndrome pCO2 – partial pressure of carbon dioxide pO2 – Partial pressure of oxygen REM – Rapid eye movement RN – Registered Nurse SaO2 – Oxygen saturation Tx – Treatment W/ - With Abbreviations
Neuronal Respiratory Control • Neuronal Control • Rhythmic cycle of breath regulated by medullary neuron interaction • Efferent activity • Cranial nerves of upper airway • Chest wall muscle innervation
Neuronal Control (cont.) • Medullary groups influenced by pontine & suprapontine descending pathways • These pathways influenced by sleep-wake cycle, particularly Reticular Activating System activity
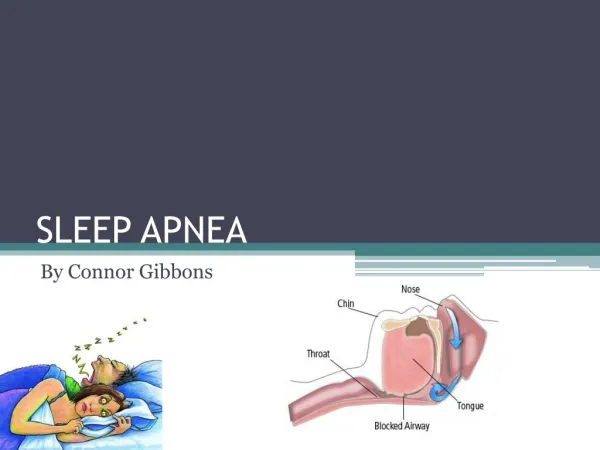
Obstructive Sleep Apnea Hypopnea - Definition • Episodes of airway obstruction during sleep resulting in recurrent arousals associated with: • Otherwise unexplained excessive daytime sleepiness AND...
Definition (cont.) • …AND > 2 of the following • Loud disruptive snoring • Nocturnal choking/gasping/snort • Recurrent nocturnal awakening • Unrefreshed sleep • Daytime fatique • Impaired concentration • ...AND... • Documented overnight sleep monitoring • >5 episodes hypopnea and apnea per hour
More Definitions • Apnea • <20% baseline airflow for 10 seconds in adults • Hypopnea • 30% baseline airflow • 10 seconds • 90% of duration of airflow 30% baseline flow • airflow accompanied by 4% oxygen saturation
Epidemiology • Overall 2-20% depending on sex and symptoms • Estimated 3 million men and 1.5 million women • M:F 2-4:1 • Daytime sleepiness 2-4% • (narcolepsy 0.02-0.06%) • Up to 85% in obese persons
History • Charles Dickens - “The Postumous Papers of the Pickwick Club” • Pickwickian Syndrome • (Obesity Hypoventilation Syndrome) • Obesity • Hypersomnolence • Signs of Chronic Alveolar Hypoventilation • Polycythemia • Sleep apnea 1 - UpToDate, 2006
Practical Predictors • HTN • History of habitual snoring • Observed reports of nocturnal choking or gasping • Neck size > 17 inches
Airway Patency • Airway size - flow resistance • Anatomic traits • Neck size • Obesity • Crowded upper airway • Large tongue • Small chin • Nasopharyngeal tumors
OSAH Etiology • Sleep affects respiratory control system • Reduced tonic input to upper airway muscles • Diminished reflexes that protect against airway collapse
Etiology (cont) • Exaggerated inspiratory effort • Decreased gas exchange • Resolves with arousal or change in sleep state
Recurrent Apnea • Instability of feedback control • Ventilation cycles instead of being maintained at a constant level
Mechanism • Sleep… • Upper airway tone... • Obstruction... • Apnea… • pO2, pCO2…
Mechanism (cont.) • …Arousal… • Upper airway tone… • Resumption of breathing… • Hyperventilation… • Return to sleep… • Upper airway tone… • This occurs HUNDREDS of times each night
Etiology (cont) • Upper airway is destablilized • Partial or complete obstruction of nasopharynx, oropharynx, or both
Presentation • Primarily relate to effects on pt’s sleep • Typically overweight men • Awaken unrested • Daytime somnolence • Disruptive snoring • 45% men & 30% women >65 yrs old snore
Sleepiness(Of course we need to define sleepiness) • Mild • Sleep during times of rest • Incidental functional impairment • Moderate • Sleep during activities requiring some attention • Concerts • Meetings • Presentations
Sleepiness (cont.) • Severe • Sleep during activities requiring at least moderate attention • Eating • Conversation • Walking • Driving • Marked functional impairment
Differential Diagnosis of Sleepiness • Sleep restriction • Narcolepsy • Restless leg syndrome • Cardiovascular, respiratory, metabolic disturbances • Drug addiction • Depression
OSAH Diagnosis-suspicion • Presentation as above • Witnessed apneic periods, nocturnal gasping or choking • >10 events per hr typical for symptomatic pts • Body habitus • HTN
Diagnosis-definitive • Nocturnal Polysomnograph • EEG • Electromyelograph • Chin • activity during REM • Limbs • checks non-respiratory causes of arousal • Electro-oculogram • Detects REM
DDx (cont.) • Nasal/oral airflow • Thoracic/abdominal movement • Oxygen saturation • Cardiac rate & rhythm • Body position
Split studies • Part 1 – Definitive diagnosis • Part 2 – Optimal CPAP level
Terms of OSA Quantification • Apnea-hypopnea index (AHI) • Apnea Index (AI) • Respiratory Disturbance Index (RDI) • Respiratory Arousal Index (RAI)
Apnea-Hypopnea Index (AHI) • # episodes apnea & hypopnea / # hrs sleep OSAH = AHI > 15 / hr
Apnea Index • # apneic episodes / # hrs sleep
Respiratory Disturbance Index (RDI) • # times per hour SaO2 drops > 3% • <5 - No OSA • 5-15 - Mild OSA • 16-30 - Moderate OSA • >30 - Severe OSA
Respiratory Arousal Index (RAI) • Computed with EEG measurement • # inspiratory associated arousals per hour of sleep
OSAH Complications • Sleepiness • Somnolence during activities • Impaired concentration • Systemic hypertension • Vascular disease
OSAH and CV Disease • Arousals – bursts of sympathetic activity • Not good • SaO2 / SaO2 causes ischemia then reperfusion • Oxydative stress • Subsequent • HTN • Insulin resistance • Inflammation • Ultimately leading to… • CV endothelial dysfunction
Other Potential Complications • Stroke • Cardiac arrhythmia • Pulmonary HTN • Morning head ache • Peri-operative complications • Impaired intubation • Impaired arousal from sedatives
Prevention • Modifiable risk factors: • Obesity • Exacerbative medications • Inadequate sleep • Modifiable complications: • Machinery/motor vehicle operation • Inform Anesthesiologist before elective procedures
Treatment - General • Depends on severity of disease • No Tx for < 15 events per hour • Behavioral Modifications
Treatment - General (Cont.) • Weight loss • 5-10% body weight may be effective • Nasal CPAP • Oral appliances
Treatment - Medical • Vasoconstrictive sprays • Weight loss meds • Oxygen (select patients) • Chemical avoidance • Sedative hypnotics • Alchohol • Antihistamines
Treatment - Surgical • Hyoplasty • Linguloplasty • Mandibular advancement • Uvulopalatopharyngoplasty • Tracheostomy
Treatment - Surgical • For loud snoring: • Laser-assisted uvuloplasty • Radiofrequency tissue ablation • May apnea and/or delay definitive treatment
Prognosis • Natural history largely unknown • IF dz progresses, it does so slowly • Implications with death: • ? in-hospital mortality d/t: • Cardiorespiratory failure • Pulmonary embolus • Case reports complications of anesthesia • Accidents • 2-7 times greater chance of MVC • Equipment operation
Central Sleep Apnea Syndrome • > 10 second cessation of breathing in the absence of respiratory effort.
Central Sleep Apnea Syndrome • Airflow stops without obstruction • Interruption of central respiratory drive • Airflow AND respiratory effort are absent • Disorder of Apneic Threshold • Relation to OSA (Mixed Apnea)
Neural disorders Poliomyelitis Posterior fossa tumors Idiopathic failure of central breathing control Complication of OSAH Narcotic induced CSAS High altitude induced periodic breathing CSAS - Etiology
CSAS – Etiology (Cont.) • Heart Failure • 37% of Pts with HF & LVEF < 45% have CSAS • 12% have OSAH
CSAS - Presentation • Insomnia • Nocturnal awakenings • Nocturnal polysomnograph • No evidence of obstruction • No respiratory movement