Download
1 / 25
300 likes | 645 Vues
Intramuscular Epinephrine Administration for the Non-Paramedic Provider. HCEC First Responder Organization Training. Goal.

E N D
Intramuscular Epinephrine Administration for the Non-Paramedic Provider HCEC First Responder Organization Training
Goal • To prepare HCEC First Responder Organization personnel to safely administer intramuscular epinephrine injections within the scope of the HCEC Fire and Rescue Medical/Trauma Guidelines
Objectives • Upon completion of the didactic and practical sections of this program, the candidate will be able to: • Identify acceptable sites of administration on the candidate’s anatomy • Correctly prepare an injection of a stated volume • Demonstrate safe administration of an intramuscular injection
Assessment • Skills will be verified using inert or expired solutions injected into an injection training model or non-living tissue under the supervision of an approved HCEC FRO Trainer • Candidates must perform the skill without critical errors as listed on the HCEC Psychomotor Skill Verification sheet for Intramuscular Medication Administration
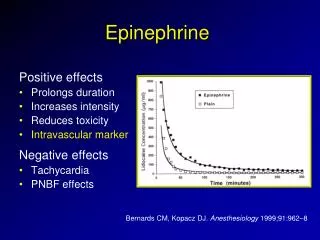
Epinephrine is an important pre-hospital medication in the treatment of asthma, anaphylaxis, and cardiac arrest.
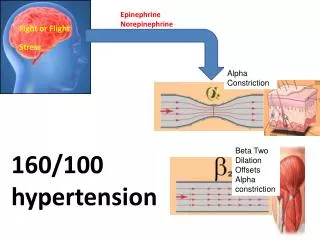
Epinephrine • Hormone and neurotransmitter endogenous to, or normally produced by, the body. • Sympathomimetic catecholamine • Stimulates the sympathetic branch of the autonomic nervous system • stimulates α1 receptors, increasing blood pressure through vasoconstriction • β1 receptors, increasing heart rate, contractile force, and myocardial oxygen demand • and β2 receptors, resulting in bronchodilation.
As an EMT-B or EMT-I you are most familiar with assisting in the administration of epinephrine by means of an epinephrine auto-injector system. • HCEC Fire and Rescue Medical/Trauma Guidelines allow for the administration of epinephrine by manual intramuscular injection for anaphylaxis by FRO EMT-B’s and EMT-Intermediates who have been trained and credentialed by the HCEC Clinical Division.
Packaging • Glass ampules - breakable glass vessels containing the liquid medication • Cone shaped top • Thin neck • Circular tubular base for storing the medication The thin neck is a vulnerable point where you intentionally break the ampule to retrieve its contents. The epinephrine used for anaphylaxis is packaged in a 1 ml ampule at a concentration of 1:1000, or 1 mg per ml.
Dosing • The adult dose of epinephrine for anaphylaxis is 0.3 mg. This is equal to 0.3 ml of 1:1000 solution. • The pediatric dose of epinephrine for anaphylaxis is 0.01 mg/kg up to a maximum of 0.3 mg per dose.
Obtaining Medication • To obtain medication from a glass ampule, you will need a syringe and needle. Use the following technique: • Confirm the medication indications and patient allergies. • Confirm the ampule label (medication name, dose, and expiration)
Obtaining Medication • Hold the ampule upright and tap its top to dislodge any trapped solution.
Obtaining Medication • Place gauze around the thin neck and snap it off with your thumb.
Obtaining Medication • Place the tip of the hypodermic needle inside the ampule and withdraw the medication into the syringe. Do not inject air into the ampule as this will expel the solution from the container.
Obtaining Medication • Properly dispose of the broken glass ampule.
Intramuscular Injections • Intramuscular injections deposit medication into muscle. Muscle is extremely vascular and permits systemic delivery at a moderate absorption rate. Drug absorption through muscle is also relatively predictable. • Intramuscular epinephrine will be delivered to the vastuslateralis muscle, along the lateral part of the thigh, midway between the waist and knee, or the deltoid muscle.
Administration • To administer the prepared epinephrine injection, use the following procedure: • Draw up the correct amount of medication using a 1 cc syringe.
Administration • Confirm the correct dose and medication. The medication should not be discolored or contaminated. You should use a 1-1 ½ inch 20-25g needle for the injection.
Administration • Prepare the injection site with an alcohol wipe or other antiseptic. Remove the needle cover.
Administration • Hold the syringe upright so any air inside rises to the base of the needle. Remove the air by gently depressing the syringe plunger.
Administration • Insert the needle quickly at a 90-degree angle to the injection site, deep enough to place the tip into the muscle beneath the skin and subcutaneous fat.
Administration • Holding the syringe steady, gently withdraw the plunger to ensure you are not in a blood vessel. If you do not get blood return, push the plunger in until it stops, to ensure that all medication is injected.
Administration • Dispose of the needle/syringe in an approved sharps container.
Reassessment and Transition of Care • Your follow-up assessment should include appearance, work of breathing, lung sounds, skin signs, vital signs, and changes in ability to speak. • Relay to the receiving medic unit: • Time and dose administered • Patient response to the medication
Adapted from: American Academy of OrthopaedicSurgeons. (2005). Allergic reactions and envenomations. In A Pollak (Ed.), Emergency care and transportation of the sick and injured (pp. 498-515). Sudbury, MA: Jones and Bartlett. Bledsoe, B.E., Porter, R.S., & Cherry, R.A. (2000). Medication administration. Paramedic care: principles & practice (pp. 366-406). Upper Saddle River, NJ: Prentice Hall.