Acute Intermittent Porphyria
400 likes | 1.93k Vues
CASE PRESENTATION. History of Present Illness. HPI: 48 year-old African American female with a remote history of schizophrenia and recently diagnosed hypertension who presents with generalized weakness that has gotten progressively worse over the past 2-3 weeks. Her weakness has become so severe t

Acute Intermittent Porphyria
E N D
Presentation Transcript
1. Acute Intermittent Porphyria
2. CASE PRESENTATION
3. History of Present Illness HPI:
48 year-old African American female with a remote history of schizophrenia and recently diagnosed hypertension who presents with generalized weakness that has gotten progressively worse over the past 2-3 weeks. Her weakness has become so severe that she cannot get out of bed, sit upright, or walk without assistance. Around the same time she also developed a tremor in her chin and hands that makes it difficult for her to hold utensils. She notes feeling lightheaded when she stands up and also complains of vague intermittent periumbilical abdominal pain.
The patient has come to the ER multiple times in the past complaining of abdominal pain, nausea, vomiting, constipation, and weakness.
PSH: BTL, Appy
No significant family or social history
Meds: Nexium, Celexa
4. Physical Exam & Laboratory Data PE:
VS: T 36.2 P 142 R 20 BP 178/112
Gen: Sleepy but arousable, AxO x3
HEENT: PERRL, EOMI, OP Clear
Neck: Supple, no LAD
CV: tachy, regular rhythm, no m/g/r
Lungs: CTAB
GI: soft, ND, mild periumbilical discomfort to palpation
Extr: no c/c/e
Skin: No rashes or skin lesion
Neuro: CN II-XII intact, strength 4/5 throughout, paresthesia in bilat lower extremities, 2+ reflexes, upgoing toes Labs:
CBC: wnl
128 94 24 9.9
110
3.8 22 1.3 1.2 2.9
LFTs: TP 7.6, Alb 3.4, AP 85,
GGT 33, AST 89, ALT 82,
TB 1.0, DB 0.3
UA � wnl
Utox -wnl
�
5. Random Problem List? Hyponatremia
Tachycardia
Hypertension
Elevated Creatinine
Abdominal Pain
Transaminitis
Weakness I want to tell you briefly about some of the main problems she had during hospital course.
Hyponatremic during hospitalization
-No evidence of adrenal insufficiency
-Her labs were consistent with SIADH, responded to fluid restriction
Tachycardia
-The pt was persistently tachy during her stay, only partially responsive to fluids (HR always 100-120)
-Sinus tachy on EKG
-No evidence of PE
-B/c of her labile HTN, pheochromocytoma r/o.
Elevated Creatinine
-Pt had large fluctuations in her Cr � often responsive to IVF but sometimes not
Abdominal Pain
-Initially c/o abd pain in the ER but later denied abdominal pain
-Negative CT Abdomen/pelvis
Transaminitis
-Negative hepatits panel
Weakness
-Talk about on next slide
Initially we thought all these problems were unrelated, but later we realized that they can be explained by one mechanism
I want to tell you briefly about some of the main problems she had during hospital course.
Hyponatremic during hospitalization
-No evidence of adrenal insufficiency
-Her labs were consistent with SIADH, responded to fluid restriction
Tachycardia
-The pt was persistently tachy during her stay, only partially responsive to fluids (HR always 100-120)
-Sinus tachy on EKG
-No evidence of PE
-B/c of her labile HTN, pheochromocytoma r/o.
Elevated Creatinine
-Pt had large fluctuations in her Cr � often responsive to IVF but sometimes not
Abdominal Pain
-Initially c/o abd pain in the ER but later denied abdominal pain
-Negative CT Abdomen/pelvis
Transaminitis
-Negative hepatits panel
Weakness
-Talk about on next slide
Initially we thought all these problems were unrelated, but later we realized that they can be explained by one mechanism
6. Random Problem List? Hyponatremia
Tachycardia
Hypertension
Elevated Creatinine
Abdominal Pain
Transaminitis
Weakness I want to tell you briefly about some of the main problems she had during hospital course.
Hyponatremic during hospitalization
-No evidence of adrenal insufficiency
-Her labs were consistent with SIADH, responded to fluid restriction
Tachycardia
-The pt was persistently tachy during her stay, only partially responsive to fluids (HR always 100-120)
-Sinus tachy on EKG
-No evidence of PE
-B/c of her labile HTN, pheochromocytoma r/o.
Elevated Creatinine
-Pt had large fluctuations in her Cr � often responsive to IVF but sometimes not
Abdominal Pain
-Initially c/o abd pain in the ER but later denied abdominal pain
-Negative CT Abdomen/pelvis
Transaminitis
-Negative hepatits panel
Weakness
-Talk about on next slide
Initially we thought all these problems were unrelated, but later we realized that they can be explained by one mechanism
I want to tell you briefly about some of the main problems she had during hospital course.
Hyponatremic during hospitalization
-No evidence of adrenal insufficiency
-Her labs were consistent with SIADH, responded to fluid restriction
Tachycardia
-The pt was persistently tachy during her stay, only partially responsive to fluids (HR always 100-120)
-Sinus tachy on EKG
-No evidence of PE
-B/c of her labile HTN, pheochromocytoma r/o.
Elevated Creatinine
-Pt had large fluctuations in her Cr � often responsive to IVF but sometimes not
Abdominal Pain
-Initially c/o abd pain in the ER but later denied abdominal pain
-Negative CT Abdomen/pelvis
Transaminitis
-Negative hepatits panel
Weakness
-Talk about on next slide
Initially we thought all these problems were unrelated, but later we realized that they can be explained by one mechanism
7. Random Problem List? Hyponatremia
Tachycardia
Hypertension
Elevated Creatinine
Abdominal Pain
Transaminitis
Weakness I want to tell you briefly about some of the main problems she had during hospital course.
Hyponatremic during hospitalization
-No evidence of adrenal insufficiency
-Her labs were consistent with SIADH, responded to fluid restriction
Tachycardia
-The pt was persistently tachy during her stay, only partially responsive to fluids (HR always 100-120)
-Sinus tachy on EKG
-No evidence of PE
-B/c of her labile HTN, pheochromocytoma r/o.
Elevated Creatinine
-Pt had large fluctuations in her Cr � often responsive to IVF but sometimes not
Abdominal Pain
-Initially c/o abd pain in the ER but later denied abdominal pain
-Negative CT Abdomen/pelvis
Transaminitis
-Negative hepatits panel
Weakness
-Talk about on next slide
Initially we thought all these problems were unrelated, but later we realized that they can be explained by one mechanism
I want to tell you briefly about some of the main problems she had during hospital course.
Hyponatremic during hospitalization
-No evidence of adrenal insufficiency
-Her labs were consistent with SIADH, responded to fluid restriction
Tachycardia
-The pt was persistently tachy during her stay, only partially responsive to fluids (HR always 100-120)
-Sinus tachy on EKG
-No evidence of PE
-B/c of her labile HTN, pheochromocytoma r/o.
Elevated Creatinine
-Pt had large fluctuations in her Cr � often responsive to IVF but sometimes not
Abdominal Pain
-Initially c/o abd pain in the ER but later denied abdominal pain
-Negative CT Abdomen/pelvis
Transaminitis
-Negative hepatits panel
Weakness
-Talk about on next slide
Initially we thought all these problems were unrelated, but later we realized that they can be explained by one mechanism
8. Random Problem List? Hyponatremia
Tachycardia
Hypertension
Elevated Creatinine
Abdominal Pain
Transaminitis
Weakness I want to tell you briefly about some of the main problems she had during hospital course.
Hyponatremic during hospitalization
-No evidence of adrenal insufficiency
-Her labs were consistent with SIADH, responded to fluid restriction
Tachycardia
-The pt was persistently tachy during her stay, only partially responsive to fluids (HR always 100-120)
-Sinus tachy on EKG
-No evidence of PE
-B/c of her labile HTN, pheochromocytoma r/o.
Elevated Creatinine
-Pt had large fluctuations in her Cr � often responsive to IVF but sometimes not
Abdominal Pain
-Initially c/o abd pain in the ER but later denied abdominal pain
-Negative CT Abdomen/pelvis
Transaminitis
-Negative hepatits panel
Weakness
-Talk about on next slide
Initially we thought all these problems were unrelated, but later we realized that they can be explained by one mechanism
I want to tell you briefly about some of the main problems she had during hospital course.
Hyponatremic during hospitalization
-No evidence of adrenal insufficiency
-Her labs were consistent with SIADH, responded to fluid restriction
Tachycardia
-The pt was persistently tachy during her stay, only partially responsive to fluids (HR always 100-120)
-Sinus tachy on EKG
-No evidence of PE
-B/c of her labile HTN, pheochromocytoma r/o.
Elevated Creatinine
-Pt had large fluctuations in her Cr � often responsive to IVF but sometimes not
Abdominal Pain
-Initially c/o abd pain in the ER but later denied abdominal pain
-Negative CT Abdomen/pelvis
Transaminitis
-Negative hepatits panel
Weakness
-Talk about on next slide
Initially we thought all these problems were unrelated, but later we realized that they can be explained by one mechanism
9. PORPHYRIA
10. Heme central to understanding Porphria Heme is part of hemoglobin, myoglobin, catalases, peroxidases, and cytochromes
Heme is made in every human cell (85% in erythroid cells & much of the rest in the liver)
First enzyme in heme synthesis pathway is ALA synthetase (ALAS)
Increase demand induces ALAS
Heme downregulates ALAS by feedback inhibition
Partial block in this pathway induces ALAS and causes accumulation of heme precursors upstream from block Before I talk about porphyria I want to mention a couple of points about heme as it is central to the disease
Heme is a vital component of hemoglobin, myoglobin, catalases, peroxidases, and cytochromes
Heme is synthesized in every human cell
-About 85% is made in erythroid cells primarily for hemoglobin formation
-Most of the remaining heme is made in the liver, 80% of which is used for the synthesis of cytochromes
First enzyme in heme synthesis pathway is Aminolevulinic acid (ALA) synthetase (ALAS)
-Usually heme pathway is tightly controlled
-ALAS is readily inducible when increased need for heme for intracellular processes
-Excess heme downregulates ALAS by feedback inhibition
-Partial block in the pathway leads to an overproduction of ALAS with accumulation of intermediates upstream from the blockBefore I talk about porphyria I want to mention a couple of points about heme as it is central to the disease
Heme is a vital component of hemoglobin, myoglobin, catalases, peroxidases, and cytochromes
Heme is synthesized in every human cell
-About 85% is made in erythroid cells primarily for hemoglobin formation
-Most of the remaining heme is made in the liver, 80% of which is used for the synthesis of cytochromes
First enzyme in heme synthesis pathway is Aminolevulinic acid (ALA) synthetase (ALAS)
-Usually heme pathway is tightly controlled
-ALAS is readily inducible when increased need for heme for intracellular processes
-Excess heme downregulates ALAS by feedback inhibition
-Partial block in the pathway leads to an overproduction of ALAS with accumulation of intermediates upstream from the block
11. Porphyria is a disruption in the heme pathway Group of metabolic diseases resulting from a partial deficiency of an enzyme in the heme biosynthetic pathway
Seven enzymes in the pathway
Four of the porphyrias cause acute attacks
Increased demand for heme can precipitate attacks secondary to overproduction of toxic heme precursors (porphyrins, ALA)
The porphyrins have no useful function and act as highly reactive oxidants damaging tissues The porphyrias are a group of metabolic diseases that result from a partial deficiency of a specific enzyme in the heme biosynthesis pathway.
There are seven enzymes in the pathway required to sythesize heme, and therefore seven different types of porphyria.
Of the seven types of porphyria, only four actually cause acute attacks.
-5-aminolevulinic acid dehydratase deficiency porphyria
-acute intermittent porphyria
-variegate porphyria
-hereditary coproporphyria
An increase in demand for heme production during times of stress can precipitate symptoms or attacks of porphyria
This is secondary to overproduction of toxic heme precursors (porphyrins) and ALA
The porphyrins have no useful function and act as highly reactive oxidants and damage tissuesThe porphyrias are a group of metabolic diseases that result from a partial deficiency of a specific enzyme in the heme biosynthesis pathway.
There are seven enzymes in the pathway required to sythesize heme, and therefore seven different types of porphyria.
Of the seven types of porphyria, only four actually cause acute attacks.
-5-aminolevulinic acid dehydratase deficiency porphyria
-acute intermittent porphyria
-variegate porphyria
-hereditary coproporphyria
An increase in demand for heme production during times of stress can precipitate symptoms or attacks of porphyria
This is secondary to overproduction of toxic heme precursors (porphyrins) and ALA
The porphyrins have no useful function and act as highly reactive oxidants and damage tissues
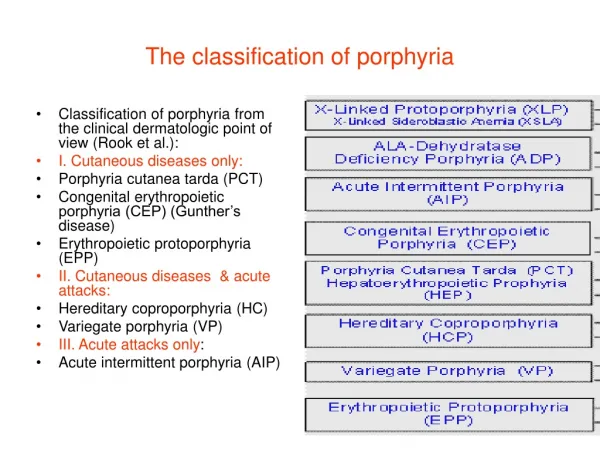
12. Overview of the Seven Porphyrias Genetic defect is autosomal dominant in most of the porphyrias, however, occasionally an autosomal recessive pattern is seen.
Multiple genetic mutations in each gene have been described
- AIP has the most # with 227 and much of the literature is littered with case reports describing these new mutations
Classified as hepatic or erythroid
- This depends on where most of the heme biosynthetic precursors (porphyrins) arise from and acummulate in
-All of the seven porphyrias are hepatic (meaning the primary enzyme defect is in the liver leading to overproduction of heme precursors in that organ) except for congenital erythropoietic porphyria and erythopoietic protoporphyria which have the defect in the red cells
Classified clinically as acute or cutaneous
- 4 of the porphyrias are acute as mentioned earlier
-All of the acute porphyrias cause neurological sx as part of the acute attacks
-Two of the acute porphyrias (VP and HCP) cause acute attacks but can also cause skin lesions (neurocutaneous)
-ADP and AIP cause attacks but no skin lesions (neuroporphyrias)Genetic defect is autosomal dominant in most of the porphyrias, however, occasionally an autosomal recessive pattern is seen.
Multiple genetic mutations in each gene have been described
- AIP has the most # with 227 and much of the literature is littered with case reports describing these new mutations
Classified as hepatic or erythroid
- This depends on where most of the heme biosynthetic precursors (porphyrins) arise from and acummulate in
-All of the seven porphyrias are hepatic (meaning the primary enzyme defect is in the liver leading to overproduction of heme precursors in that organ) except for congenital erythropoietic porphyria and erythopoietic protoporphyria which have the defect in the red cells
Classified clinically as acute or cutaneous
- 4 of the porphyrias are acute as mentioned earlier
-All of the acute porphyrias cause neurological sx as part of the acute attacks
-Two of the acute porphyrias (VP and HCP) cause acute attacks but can also cause skin lesions (neurocutaneous)
-ADP and AIP cause attacks but no skin lesions (neuroporphyrias)
13. Overview of the Four Acute Porphyrias Four acute porphyrias cause acute, self-limiting attacks that lead to chronic and progressive deficits
Symptoms of acute attacks mimic other diseases and increase the potential for misdiagnosis.
Acute porphyrias are clinically indistinguishable during acute attacks, except the neurocutaneous porphyrias (variegate porphyria and hereditary coproporphyria) can cause dermatologic changes
Acute attacks lead to an increase in porphobilinogen (PBG) and 5-aminolevulinic acid (ALA) which can be detected in the urine
Things that make diagnosis difficult: variable clinic course, lack of understanding about diagnostic process, and lack of a universal standard for test result interpretation Four acute porphyrias cause acute, self-limiting attacks that lead to chronic and progressive deficits
Symptoms of acute attacks mimic other diseases and increase the potential for misdiagnosis.
Acute porphyrias are clinically indistinguishable during acute attacks, except the neurocutaneous porphyrias (variegate porphyria and hereditary coproporphyria) can cause dermatologic changes
Acute attacks arise after puberty and occur more frequently in women
Acute attacks lead to an increase in porphobilinogen (PBG) and 5-aminolevulinic acid (ALA) which can be detected in the urine
Things that make diagnosis difficult: variable clinic course, lack of understanding about diagnostic process, and lack of a universal standard for test result interpretationFour acute porphyrias cause acute, self-limiting attacks that lead to chronic and progressive deficits
Symptoms of acute attacks mimic other diseases and increase the potential for misdiagnosis.
Acute porphyrias are clinically indistinguishable during acute attacks, except the neurocutaneous porphyrias (variegate porphyria and hereditary coproporphyria) can cause dermatologic changes
Acute attacks arise after puberty and occur more frequently in women
Acute attacks lead to an increase in porphobilinogen (PBG) and 5-aminolevulinic acid (ALA) which can be detected in the urine
Things that make diagnosis difficult: variable clinic course, lack of understanding about diagnostic process, and lack of a universal standard for test result interpretation
14. Patient Focus: Acute Intermittent Porphyria Most common porphyria
Deficiency of hepatic PBG deaminase
Autosomal dominant pattern with incomplete penetrance
Affected individuals have a 50% reduction in erythrocyte PBG deaminase activity
Latent prior to puberty
Symptoms more common in females than males
Increased urinary ALA & PBG Most common porphyria
Deficiency of hepatic (And Erythrocyte) PBG deaminase
-Varient form of AIP with normal Erythrocyte PBG deaminase activity
Autosomal dominant pattern with incomplete penetrance
Affected individuals have a 50% reduction in erythrocyte PBG deaminase activity
Latent prior to puberty
Symptoms more common in females than males
Increased urinary ALA and PBG
-The acute forms of the disease cause concomitant failure of PBG deaminase to respond appropriately
-ALA accumulation i(in the acute porphyrias other than ALA Dehydratase Def)
-inhibitory affect of PBG on ALA dehydratase
-ALA dehydratase is upregulated in response to deficiency of heme
Most common porphyria
Deficiency of hepatic (And Erythrocyte) PBG deaminase
-Varient form of AIP with normal Erythrocyte PBG deaminase activity
Autosomal dominant pattern with incomplete penetrance
Affected individuals have a 50% reduction in erythrocyte PBG deaminase activity
Latent prior to puberty
Symptoms more common in females than males
Increased urinary ALA and PBG
-The acute forms of the disease cause concomitant failure of PBG deaminase to respond appropriately
-ALA accumulation i(in the acute porphyrias other than ALA Dehydratase Def)
-inhibitory affect of PBG on ALA dehydratase
-ALA dehydratase is upregulated in response to deficiency of heme
15. Prevalence in the General Population United States: ~ 1 in 10,000-20,000
However, clinical disease manifests itself in approximately 10% of these carriers
Finland & Western Australia: ~ 3 in 100,000
Sweden: ~ 1 in 10,000
Highest prevalence
NOTE: Incidence of acute intermittent porphyria is higher in the psychiatric population compared with the general population In the U.S. the prevalence is 1 in 10,000-20,000, however, clinical disease manifests itself in approximately 10% of these carriers
Prevalence is 3 in 100,000 in Finland and Western Australia
In Sweden, the gene prevalence is highest - about 1 per 10,000
The incidence of AIP is higher in the psychiatric population compared with the general populationIn the U.S. the prevalence is 1 in 10,000-20,000, however, clinical disease manifests itself in approximately 10% of these carriers
Prevalence is 3 in 100,000 in Finland and Western Australia
In Sweden, the gene prevalence is highest - about 1 per 10,000
The incidence of AIP is higher in the psychiatric population compared with the general population
16. Key Clinical Features Gastrointestinal symptoms - Abdominal pain (most common presenting complaint), nausea/vomiting, constipation, and diarrhea.
Dehydration
Hyponatremia
Cardiovascular symptoms - tachycardia, hypertension, arrhythmias
Neurologic manifestations - motor neuropathy, sensory neuropathy, mental symptoms, seizures. AIP is exculsively neuropsychiatric without any cutaneous findings
Gastrointestinal symptoms:
-Abdominal pain (most common presenting complaint)
-Abd exam is relatively benign considering symptom severity
-Pain is severe, constant and can occur in any quadrant (epigastrum is most common) It is thought to be
-Pain 2/2 autonomic neuropathy & also maybe component of abnormal bowel function with alternating areas of spastic and relaxed bowel
-nausea/vomiting
-constipation
Dehydration
Hyponatremia �
-Unclear mechanism � 2/2 to SIADH
-excess renal sodium excretion &
-damage to the supraoptic nuclei of the hypothalamus
-It can lead to seizures
Autonomic instability �
-Tachycardia is a frequent physical finding during acute attacks
-Catecholamine release is increased during acute attacks and may contribute to sudden death 2/2 cardiac arrhythmias
Confusion and stupor
Seizures (lower seizure threshold unrelated to hyponatremia)
Neuro manifestations
-Motor neuropathy (may resemble a Guillain-Barre syndrome)
-muscle weakness that usually begins proximally; usually in the upper rather than lower extremities; which can lead to cranial nerve impairment, and bulbar muscle paralysis
-Sensory neuropathy in a �bathing trunk� distribution with pain over trunk and thighs
-Mental symptoms -- behavioral changes, agitation, confusion, hallucinations, and depression (can resolve when acute attack over)AIP is exculsively neuropsychiatric without any cutaneous findings
Gastrointestinal symptoms:
-Abdominal pain (most common presenting complaint)
-Abd exam is relatively benign considering symptom severity
-Pain is severe, constant and can occur in any quadrant (epigastrum is most common) It is thought to be
-Pain 2/2 autonomic neuropathy & also maybe component of abnormal bowel function with alternating areas of spastic and relaxed bowel
-nausea/vomiting
-constipation
Dehydration
Hyponatremia �
-Unclear mechanism � 2/2 to SIADH
-excess renal sodium excretion &
-damage to the supraoptic nuclei of the hypothalamus
-It can lead to seizures
Autonomic instability �
-Tachycardia is a frequent physical finding during acute attacks
-Catecholamine release is increased during acute attacks and may contribute to sudden death 2/2 cardiac arrhythmias
Confusion and stupor
Seizures (lower seizure threshold unrelated to hyponatremia)
Neuro manifestations
-Motor neuropathy (may resemble a Guillain-Barre syndrome)
-muscle weakness that usually begins proximally; usually in the upper rather than lower extremities; which can lead to cranial nerve impairment, and bulbar muscle paralysis
-Sensory neuropathy in a �bathing trunk� distribution with pain over trunk and thighs
-Mental symptoms -- behavioral changes, agitation, confusion, hallucinations, and depression (can resolve when acute attack over)
17. Pathophysiology of the Acute Attack Symptoms during an acute attack are thought to be secondary to accumulation of porphyrin precursors rather than from deficiency of heme
Massive amounts of porphyrins are excreted from the liver
Porphyrins are neurotoxic and affect areas of the nervous system not protected by blood-brain barrier
-Autonomic Nervous System
-Peripheral Nervous System
-hypothalamus
-limbic area
It has also been proposed that accumulation of ALA may lead to neurological symptoms by crossing the blood-brain barrier and accumulating in the brain ? ALA has a pro- oxidative effect with generation ROS which cause neuronal and glial cell damage
In addition, ALA accumulates in the liver and can cause liver damage through these oxidative effectsSymptoms during an acute attack are thought to be secondary to accumulation of porphyrin precursors rather than from deficiency of heme
Massive amounts of porphyrins are excreted from the liver
Porphyrins are neurotoxic and affect areas of the nervous system not protected by blood-brain barrier
-Autonomic Nervous System
-Peripheral Nervous System
-hypothalamus
-limbic area
It has also been proposed that accumulation of ALA may lead to neurological symptoms by crossing the blood-brain barrier and accumulating in the brain ? ALA has a pro- oxidative effect with generation ROS which cause neuronal and glial cell damage
In addition, ALA accumulates in the liver and can cause liver damage through these oxidative effects
18. Exacerbating Factors of Acute Attack Drugs that increase demand for hepatic heme (especially cytochrome P450 enzymes)
Crash diets (decrease carbohydrate intake)
Endogenous hormones (progesterone)
Cigarette smoking (induces cytochrome P450)
Metabolic stresses (infections, surgery, psychological stress) Drugs that increase demand for hepatic heme (especially cytochrome P450 enzymes)
Crash diets (decrease carbohydrate intake)
Endogenous hormones (progesterone)
Cigarette smoking (induces cytochrome P450)
Metabolic stresses (infections, surgery, psychological stress)
Drugs that increase demand for hepatic heme (especially cytochrome P450 enzymes)
Crash diets (decrease carbohydrate intake)
Endogenous hormones (progesterone)
Cigarette smoking (induces cytochrome P450)
Metabolic stresses (infections, surgery, psychological stress)
20. Diagnosis of Acute Porphyria Initial testing with rapid urinary PBG testing (Ex: Watson-Schwartz, Trace PBG Kit)
PBG Qualitative � **POSITIVE**
Confirm with quantitative PBG and ALA testing (Acute attacks: urinary PBG 20-200 mg/d)
PBG 118 mg/24 hrs (0-4 mg/d)
ALA 18.8 mg/24hrs (0-7 mg/d)
If only ALA is elevated (and not PBG), then ALA dehydratase deficiency porphyria should be considered
Note: Urinary PBG may not be substantially elevated if pt already receiving treatment with hemin
Porphyria should be considered in patients with symptoms that are prominent in this condition
- Especially in patients with no other identifiable cause (EX abdominal pain with negative workup)
- 5-10% of patients may not have the most common features making diagnosis more difficult
- Usually family history is not helpful as most carriers are asymptomatic (this was true in our pt)
Can screen initially with rapid urinary PBG testing (Watson-Schwartz)
- This test is qualitative, rapid, and readily available (POSITIVE IN OUR PATIENT)
-Test is not very sensitive with common false positive tests (therefore followed by quantitative test)
-Next need to confirm dx with quantitative PBG and ALA levels (BOTH ELEVATED IN OUR PATIENT)
If only ALA is elevated (and not PBG), then ALA dehydratase def should be considered
If ADP suspected, need to rule out other causes of ALA- dehydratase deficiency including lead poisoning and hereditary tyrosinemia type I which can cause similar sx to porphyria
Once diagnosis of porphyria is made based on the above tests, the type of porphyria can be determined by measuring individual porphyrin levels in the urine, plasma, and feces
-Porphyrins in the urine and feces are separated out by (HPLC) High Performance Liquid Chromatography
-Plasma porphyrins are meausured through fluorometryPorphyria should be considered in patients with symptoms that are prominent in this condition
- Especially in patients with no other identifiable cause (EX abdominal pain with negative workup)
- 5-10% of patients may not have the most common features making diagnosis more difficult
- Usually family history is not helpful as most carriers are asymptomatic (this was true in our pt)
Can screen initially with rapid urinary PBG testing (Watson-Schwartz)
- This test is qualitative, rapid, and readily available (POSITIVE IN OUR PATIENT)
-Test is not very sensitive with common false positive tests (therefore followed by quantitative test)
-Next need to confirm dx with quantitative PBG and ALA levels (BOTH ELEVATED IN OUR PATIENT)
If only ALA is elevated (and not PBG), then ALA dehydratase def should be considered
If ADP suspected, need to rule out other causes of ALA- dehydratase deficiency including lead poisoning and hereditary tyrosinemia type I which can cause similar sx to porphyria
Once diagnosis of porphyria is made based on the above tests, the type of porphyria can be determined by measuring individual porphyrin levels in the urine, plasma, and feces
-Porphyrins in the urine and feces are separated out by (HPLC) High Performance Liquid Chromatography
-Plasma porphyrins are meausured through fluorometry
21. Steps to Confirm Acute Intermittent Porphyria Diagnosis Determine type of porphyria by measuring individual porphyrin levels in the urine, feces, and plasma (by chromatography & fluorometry)
Confirmation of diagnosis = erythrocyte PBG deaminase activity (only 50% of the normal activity)
DNA testing for patients & at-risk family members (mutations usually family-specific)
Do NOT wait for results of secondary testing prior to treatment
-When looking at the fractionated porphyrin levels it is best to focus on which porphyrins predominate, rather than to focus on the absolute levels of each porphyrin
-In AIP fractionated porphyrin analysis in the urine shows a relative increase in uroporphyrin with only normal or
only slightly elevated fecal/plasma porphyrins
Coproporphyrin is the predominant porphyrin in normal urine and is also excreted in the bile
-An increase in urinary coproporphyrin levels can increase in lead poisoning, bone marrow disorders, and liver disease (even minor liver dysfunction can cause increased urinary coproporphyrin excretion) ?
-In our patient she initially was seen to have elevated coproporphyrin which could have been secondary to her elevated LFTs.
-Therefore, urinary elevation of porphyrins is nonspecific (esp coproporphyrin) if not in combination with elevations in PBG and ALA.
Measurement of PBG in the serum is useful when acute porphyria is suspected but urine cannot be collected (for ex in renal failure)
Definitive Diagnosis is made by measuring enzyme activity (50% normal level of erythrocyte PBG deaminase activity) and doing DNA testing.
However, it is possible to have normal erythrocyte PBG deaminase but still have AIP with low PGB deaminase in the liver and in other cells.
In addition, there is a wide range of normal enzyme activity for PBG deaminase therefore low-normal values and high-carrier values can overlap, also there is increased enzyme activity in younger erythrocytes, and improper processing, storing, and shipping of blood samples can decrease enzyme activity.
PBG/ALA levels usually remain high after acute attack in AIP but decrease after acute attack in HCP and VP
Do NOT wait for results of secondary testing prior to treatment
-When looking at the fractionated porphyrin levels it is best to focus on which porphyrins predominate, rather than to focus on the absolute levels of each porphyrin
-In AIP fractionated porphyrin analysis in the urine shows a relative increase in uroporphyrin with only normal or
only slightly elevated fecal/plasma porphyrins
Coproporphyrin is the predominant porphyrin in normal urine and is also excreted in the bile
-An increase in urinary coproporphyrin levels can increase in lead poisoning, bone marrow disorders, and liver disease (even minor liver dysfunction can cause increased urinary coproporphyrin excretion) ?
-In our patient she initially was seen to have elevated coproporphyrin which could have been secondary to her elevated LFTs.
-Therefore, urinary elevation of porphyrins is nonspecific (esp coproporphyrin) if not in combination with elevations in PBG and ALA.
Measurement of PBG in the serum is useful when acute porphyria is suspected but urine cannot be collected (for ex in renal failure)
Definitive Diagnosis is made by measuring enzyme activity (50% normal level of erythrocyte PBG deaminase activity) and doing DNA testing.
However, it is possible to have normal erythrocyte PBG deaminase but still have AIP with low PGB deaminase in the liver and in other cells.
In addition, there is a wide range of normal enzyme activity for PBG deaminase therefore low-normal values and high-carrier values can overlap, also there is increased enzyme activity in younger erythrocytes, and improper processing, storing, and shipping of blood samples can decrease enzyme activity.
PBG/ALA levels usually remain high after acute attack in AIP but decrease after acute attack in HCP and VP
22. Fractionated Porphyrins Suggest Acute Intermittent Porphria in Our Patient Fractionated Porphyrins: (6 months later - After Resolution of Acute Attack)
�
Uroporphyrin I 1428 ug/24h (<120)
Uroporphyrin III 804 ug/24h (<50)
Heptacarboxyl I 28 ug/24h (<40)
Heptacarboxyl III 77 ug/24h (<40)
Isoheptacarboxyl 13 ug/24h (<30)
Hexacarboxyl I 7 ug/24h (<10)
Hexacarboxyl III 27 ug/24h (<10)
Isohexacarboxyl 50 ug/24h (<10)
Pentacarboxyl I 78 ug/24h (<20)
Pentacarboxyl III 23 ug/24h (<20)
Isopentacarboxyl 144 ug/24h (<80)
Coproporphyrin I 438 ug/24h (<500)
Coproporphyrin III 175 ug/24h (<400)
Isocoproporphyrins 151 ug/24h (<200)
Protoporphyrin 421 ug/24h (<1500)
� We meausured fractionated urinary porphyrins in our patient
Our patient primarily had elevation of uroporphyrin on urinary porphyrin fractionation which is suggestive of AIP
ALA Dehydratase 6.0 nmol/L (>4.0)
Zinc-Complexed Protoporphyrin 56 mcg/dL (10-38)
We meausured fractionated urinary porphyrins in our patient
Our patient primarily had elevation of uroporphyrin on urinary porphyrin fractionation which is suggestive of AIP
ALA Dehydratase 6.0 nmol/L (>4.0)
Zinc-Complexed Protoporphyrin 56 mcg/dL (10-38)
23. Algorithm for Acute Porphyria Diagnosis
24. Treatment of the Acute Attack Hospitalization to control/treat acute symptoms:
Seizures � Seizure precautions, medications?
Electrolyte abnormalities
Dehydration / hyponatremia
Abdominal Pain � narcotic analgesics
Nausea/vomiting � phenothiazines
Tachycardia/hypertension � Beta blockers
Urinary retention / ileus
Withdraw all unsafe medications
Monitor respiratory function, muscle strength, neurological status
Mild attacks (no paresis or hyponatremia) � Intravenous 10% glucose at least 300 g per day
Severe attacks � Intravenous hemin (3-4 mg/kg qdaily for 4 days) ASAP (can give IV glucose while waiting for IV hemin)
Cimetidine for treatment of crisis and prevention of attacks Hospitalization to control/treat acute symptoms:
Seizures � Seizure precautions (many antiseizure meds unsafe � can use benzo�s, gabapentin, and vigabatrin)
Electrolyte abnormalities
Dehydration/hyponatremia
Abdominal Pain � narcotic analgesics
Nausea/vomiting � phenothiazines
Tachycardia/hypertension � Beta blockers
Withdraw all unsafe medications
Monitor respiratory function, muscle strength, neurological status (can have respiratory muscle weakness)
Mild attacks (no paresis or hyponatremia) � Intravenous 10% glucose at least 300 g per day
- Some early studies have shown that oral/IV carbohydrate loading may repress hepatic ALA synthase and therefore decrease symptoms during acute attacks.
- This used to be the treatment of choice prior to the introduction of IV hemin in 1971
Severe attacks � Intravenous hemin (3-4 mg qdaily for 4 days) ASAP (can give IV glucose while waiting for IV hemin)
- Hemin represses hepatic ALA synthase activity and decreases overproduction of ALA and PBG by at least temporarily replenishing the heme pool
- Limited studies done examining hemin � multiple uncontrolled studies and only one double-blind placebo controlled trial done ? large decreases in urine PBG excretion and decreased symptoms of acute attack with its use; (low statistical power of study 2/2 small sample size)
- 4 day course costs $8000
- S/E�s of hemin include phlebitis, anticoagulation effect, fever, aching, malaise, hemolysis
- Heme arginate (not available in U.S.
- In rare instances where pts have severe, unremitting symptomatic disease, orthotopic liver transplantation has been done
Cimetidine for treatment of crisis and prevention of attacks
-There are cases report of IV Cimetidine 900-1200 mg/day for acute crisis with improvement in sx within 48-72 hours with decrease in urinary PBG excretion
-It was also given prophylactically to prolong periods of remission with a dose of 400-800 mg PO daily with periods of prolonged remission
Hospitalization to control/treat acute symptoms:
Seizures � Seizure precautions (many antiseizure meds unsafe � can use benzo�s, gabapentin, and vigabatrin)
Electrolyte abnormalities
Dehydration/hyponatremia
Abdominal Pain � narcotic analgesics
Nausea/vomiting � phenothiazines
Tachycardia/hypertension � Beta blockers
Withdraw all unsafe medications
Monitor respiratory function, muscle strength, neurological status (can have respiratory muscle weakness)
Mild attacks (no paresis or hyponatremia) � Intravenous 10% glucose at least 300 g per day
- Some early studies have shown that oral/IV carbohydrate loading may repress hepatic ALA synthase and therefore decrease symptoms during acute attacks.
- This used to be the treatment of choice prior to the introduction of IV hemin in 1971
Severe attacks � Intravenous hemin (3-4 mg qdaily for 4 days) ASAP (can give IV glucose while waiting for IV hemin)
- Hemin represses hepatic ALA synthase activity and decreases overproduction of ALA and PBG by at least temporarily replenishing the heme pool
- Limited studies done examining hemin � multiple uncontrolled studies and only one double-blind placebo controlled trial done ? large decreases in urine PBG excretion and decreased symptoms of acute attack with its use; (low statistical power of study 2/2 small sample size)
- 4 day course costs $8000
- S/E�s of hemin include phlebitis, anticoagulation effect, fever, aching, malaise, hemolysis
- Heme arginate (not available in U.S.
- In rare instances where pts have severe, unremitting symptomatic disease, orthotopic liver transplantation has been done
Cimetidine for treatment of crisis and prevention of attacks
-There are cases report of IV Cimetidine 900-1200 mg/day for acute crisis with improvement in sx within 48-72 hours with decrease in urinary PBG excretion
-It was also given prophylactically to prolong periods of remission with a dose of 400-800 mg PO daily with periods of prolonged remission
25. Hematin (Panhematin) Used in the treatment of the acute porphyrias since the 1970s
Mechanism of Action: Reduces production of ALA / porphyrins by negative feedback inhibition on ALA synthetase
Derived from outdated PRBCs from community blood banks
Reconstitution of lyophilized hematin with 25% albumin recommended
Reconstituted in sterile water originally �> less stable / degraded easily
Degradation products cause an ? in adverse reactions
Adverse reactions: Due to degradation products binding to endothelial cells, platelets, & coagulation factors
Thrombophlebitis
Anticoagulation (transient ? PT, bleeding may occur)
Thrombocytopenia
Goetsch and Bissell in an animal model showed that fresh hematin suppressed porphyrin production whereas aged hematin did not
In vitro, fresh hematin added to human plasma produced lower PTs compared to aged hematin and hematin stored at higher temp
Anticoagulation effect mostly resolves at 5 hours and completely resolves at 48 hours
Hematin binds protiens and inhbits clotting factor fxn and fibrinolysis (Siegert & Holt)
Upregulation of oxgenase-1 & replenishment of the heme pool
Goetsch and Bissell in an animal model showed that fresh hematin suppressed porphyrin production whereas aged hematin did not
In vitro, fresh hematin added to human plasma produced lower PTs compared to aged hematin and hematin stored at higher temp
Anticoagulation effect mostly resolves at 5 hours and completely resolves at 48 hours
Hematin binds protiens and inhbits clotting factor fxn and fibrinolysis (Siegert & Holt)
Upregulation of oxgenase-1 & replenishment of the heme pool
26. Hematin (continued) ? thrombophlebitis if given through large vein or central line
Dosing:
Acute attacks: 3-4 mg/kg/day x 4 or more days
Max daily dose 6 mg/kg or 313 mg (1 vial) � even in obese patients
Prevention of attacks: not well established; once or twice weekly infusions
It has not been established whether or not preventive therapy is effective..sometimes once / twice weekly infusion can be done (especially during premenstrual period for women)
Twice daily dosing likely not more effective than qday dosing
Cleared hepatically
It has not been established whether or not preventive therapy is effective..sometimes once / twice weekly infusion can be done (especially during premenstrual period for women)
Twice daily dosing likely not more effective than qday dosing
Cleared hepatically
27. A Study of Hemin Use in Clinical Practice Hemin approved under Orphan Drug Act of 1983
Hemin removed from market in 2000 by FDA: 8/00-6/01
Abbott Laboratories required to conduct open-label study of the safety of hemin manufactured at a new facility
Largest trial / case series to date on hemin therapy
Study design: �Real world� data about acute porphyria diagnosis, treatment & perceived efficacy of treatment
Methods:
Hemin only available through study participation � compassionate basis
All pts judged to need hemin by their physicians were enrolled
Confirmation of diagnosis not required
Pts received hemin as normally prescribed by their physicians
No specific outcome measures, exclusion criteria, or follow-up
28. Results of Hemin Used in Clinical Practice Study Population: 130 pts; 92% Caucasian; 72% female
Precipitating factors: (40/130 pts): drugs (22%); hormonal (24%)
Results:
111 pts treated for 305 acute attacks & 40 pts for prophylaxis
Diagnostic lab findings reported in 53% (<half with +results)
Hemin regarded as effective for 73% of patients
Despite doses less than recommended in 20% of pts (< 3-4 mg/kg/day)
Propylaxis with hemin in 1/3 of patients
Wide variability in prophylaxis regimens ? lack of published guidelines
Among 31 receiving hemin prophylaxis for >1 month, 68% did not require subsequent tx for acute attacks
44% of pts experienced adverse events � most attributed to underlying disease and not hemin
Phlebitis was most common adverse event attributed to hematin
29. Long-Term Complications from Symptomatic Disease Neurological Sequelae
Hypertension
Renal failure
Cirrhosis
Hepatocellular carcinoma
Neurological Sequelae � chronic neurological damage if acute attack tx delayed
Hypertension
Renal failure
-Previously, abnormal renal function in AIP pts has been attributed to HTN, but this is still not certain
-However, there have been case reports of renal failure preceding the onset of HTN
-A population-based study done in Sweden examining renal function in AIP pts examined 16 pts without any other cause for renal failure (14 of these pts had HTN also). Renal bx showed diffuse glomerulosclerotic and interstitial changes with additional ischemic lesions (possibly 2/2 protracted vasospasm)
-Increased risk of HTN and renal failure in pts with acute attacks/symptoms ? proposed that excessive amounts of porphyrin metabolites could be the cause of cytoxic or vasospastic renal vascular lesions, thereby inducing HTN acutely and chronically.
-Also, increased urinary excretion of catecholamines during an acute attack from stimulation of the sympathetic nervous system may also lead to vasospasm
Hepatocellular carcinoma
-One study estimated that there is a 61-fold increased risk for HCC in AIP patients
-A retrospective population-based mortality study done in Sweden found that HCC was found in 27% of pts with AIP versus 0.2% of the deceased non-AIP patients. HCC was found to be more common in women (2:1) and in AIP pts with history of symptomatic disease versus those without. They also found that liver cirrhosis was more common in AIP pts (12%) esp women, compared with controls.
-There is no established reason for this risk, but it is felt to be 2/2 the oxidative action of ALA that can induce DNA damage by generation of reactive oxygen species
-Also, a reduced free heme pool could adversely affect cytochrome P450 and important antioxidant enzymes, leading to an increase in reactive oxygen species.
-In addition, ALA promotes release of iron from ferritin in the liver ? it is proposed that this could lead to iron overload which could increase risk of HCC
Neurological Sequelae � chronic neurological damage if acute attack tx delayed
Hypertension
Renal failure
-Previously, abnormal renal function in AIP pts has been attributed to HTN, but this is still not certain
-However, there have been case reports of renal failure preceding the onset of HTN
-A population-based study done in Sweden examining renal function in AIP pts examined 16 pts without any other cause for renal failure (14 of these pts had HTN also). Renal bx showed diffuse glomerulosclerotic and interstitial changes with additional ischemic lesions (possibly 2/2 protracted vasospasm)
-Increased risk of HTN and renal failure in pts with acute attacks/symptoms ? proposed that excessive amounts of porphyrin metabolites could be the cause of cytoxic or vasospastic renal vascular lesions, thereby inducing HTN acutely and chronically.
-Also, increased urinary excretion of catecholamines during an acute attack from stimulation of the sympathetic nervous system may also lead to vasospasm
Hepatocellular carcinoma
-One study estimated that there is a 61-fold increased risk for HCC in AIP patients
-A retrospective population-based mortality study done in Sweden found that HCC was found in 27% of pts with AIP versus 0.2% of the deceased non-AIP patients. HCC was found to be more common in women (2:1) and in AIP pts with history of symptomatic disease versus those without. They also found that liver cirrhosis was more common in AIP pts (12%) esp women, compared with controls.
-There is no established reason for this risk, but it is felt to be 2/2 the oxidative action of ALA that can induce DNA damage by generation of reactive oxygen species
-Also, a reduced free heme pool could adversely affect cytochrome P450 and important antioxidant enzymes, leading to an increase in reactive oxygen species.
-In addition, ALA promotes release of iron from ferritin in the liver ? it is proposed that this could lead to iron overload which could increase risk of HCC
30. Renal failure: Is hypertension the cause or the effect Debate about cause: Hypertension or another etiology?
Increased risk of renal failure in those with more acute attacks
Andersson et al ? Population-based study (Sweden)
Renal biopsies (n=16) ? ischemic lesions, ? related to protracted vasospasm
Theory of injury ? Vasospasm from:
Porphyrin metabolites &
an upregulated SNS ? ? urinary excretion of catecholamines during an acute attack
By this theory, hypertension is not the sole cause of renal insufficiency diffuse glomerulosclerotic and interstitial changes with additional ischemic lesions (possibly 2/2 protracted vasospasm)diffuse glomerulosclerotic and interstitial changes with additional ischemic lesions (possibly 2/2 protracted vasospasm)
31. Hepatocellular Carcinoma (HCC) Estimated 60 to 70-fold ? risk of HCC in AIP patients
Andersson ? Retrospective population-based mortality study
HCC ? 27% with AIP vs 0.2% deceased without AIP
HCC more common in women (2:1)
HCC more common in those with symptomatic disease
Cirrhosis more common in AIP pts (12%) vs non-AIP (0.5%)
Cirrhosis in AIP pts higher in W>M 3:1
Retrospective analysis for genetic mutations in 17 pts with AIP & HCC (L Bjersing)
Is PBGD a tumor suppressor gene? (No, 1 allele present in tumor)
No mutations seen in p53 or ras (these mutations have been implicated in HCC caused by HBV or aflatoxin) 2122 pts (33 with AIP) � C Andersson
One study estimated that there is a 61-fold increased risk for HCC in AIP patients
ALA promotes release of iron from ferritin in the liver ? may lead to iron overload which could increase risk of HCC
2122 pts (33 with AIP) � C Andersson
One study estimated that there is a 61-fold increased risk for HCC in AIP patients
ALA promotes release of iron from ferritin in the liver ? may lead to iron overload which could increase risk of HCC
32. Hepatocellular Carcinoma (continued) De Siervi et al ? ALA is toxic to two hepatocellular cancer cell lines (HEP G2 & HEP 3B)
Degree of cytotoxicity was directly related to concentration of ALA
Adding hemin or D-glucose to ALA + cells decreased toxicity with HEP G2 cells
Proposed Mechanism of cirrhosis / carcinogenesis:
Reduced free heme pool ? ? cytochrome P450 & antioxidant enzymes ? ? reactive oxygen species ? DNA damage
ALA that accumulates can oxidize proteins & cause DNA damage
33. Prevention & Follow-up: Caring for Patients Between Attacks Avoidance of alcohol, smoking, and exacerbating drugs
Adequate carbohydrate intake
Medical alert bracelets/wallet cards
Gonadotropin-releasing hormone analogues
Iron overload from hemin (100 mg of hemin contains 8 mg of iron)
Hepatocellular carcinoma screening
End-Stage renal disease prevention
Screening for Osteoporosis
? risk from GNRH analogues, immobility, malnutrition, & vitamin D deficiency
Avoidance of alcohol, smoking, and exacerbating drugs
Adequate carbohydrage intake
Medical alert bracelets/wallet cards
Gonadotropin-releasing hormone analogues
- Thought to be primarily secondary to progesterone (induces heme synthesis in the liver)
- Can be used in women who have acute attacks during the luteal phase of their menstrual cycle
- Eventually a low-dose estrogen patch can be added to prevent menopausal symptoms
- Need Gyn f/u and bone density tests every 6 months
- Although pregnancy increased progesterone, most women can tolerate (if acute attacks, hemin is safe during pregnancy)
Iron Overload from hemin
- Theoretically risk 2/2 frequent hemin administration (100 mg hemin = 8 mg Fe)
- Monitor ferritin levels
Hepatocellular Carcinoma Screening
periodic screening with RUQ Ultrasound and AFP levels)
- Higher incidence of HCC than in the general population seen in various studies � up to 60 to 70 fold increase
End-Stage Renal Disease Prevention
- May be partially due to uncontrolled chronic HTN, therefore, good BP control necessaryAvoidance of alcohol, smoking, and exacerbating drugs
Adequate carbohydrage intake
Medical alert bracelets/wallet cards
Gonadotropin-releasing hormone analogues
- Thought to be primarily secondary to progesterone (induces heme synthesis in the liver)
- Can be used in women who have acute attacks during the luteal phase of their menstrual cycle
- Eventually a low-dose estrogen patch can be added to prevent menopausal symptoms
- Need Gyn f/u and bone density tests every 6 months
- Although pregnancy increased progesterone, most women can tolerate (if acute attacks, hemin is safe during pregnancy)
Iron Overload from hemin
- Theoretically risk 2/2 frequent hemin administration (100 mg hemin = 8 mg Fe)
- Monitor ferritin levels
Hepatocellular Carcinoma Screening
periodic screening with RUQ Ultrasound and AFP levels)
- Higher incidence of HCC than in the general population seen in various studies � up to 60 to 70 fold increase
End-Stage Renal Disease Prevention
- May be partially due to uncontrolled chronic HTN, therefore, good BP control necessary
34. Prognosis Prior to 1970, fatality rates were 10% to 52%, now 10%
Since introduction of hematin mortality has decreased
Overall mortality in patients with acute attacks is 3-fold higher than the general population
Delayed diagnosis and treatment contribute to higher mortality Prior to 1970, fatality rates were 10% to 52%, now 10%
Since introduction of hematin mortality has decreased (one study reported about 14%)
Overall mortality in patients with acute attacks is 3-fold higher than the general population
Delayed diagnosis and treatment contribute to higher mortality
Prior to 1970, fatality rates were 10% to 52%, now 10%
Since introduction of hematin mortality has decreased (one study reported about 14%)
Overall mortality in patients with acute attacks is 3-fold higher than the general population
Delayed diagnosis and treatment contribute to higher mortality
35. Future Treatment Directions Liver transplantation
Animal models used to mimic porphyrias with experiments to correct enzyme deficiency in tissues
Non-viral mediated gene transfers There have been some cases of liver transplantation in pts with severe porphyria with frequent disabling attacks ? one study of a 19 year-old women had a liver transplant with normalized urine porphyrin excretion and resolution of her acute attacks.
Animal models used to mimic porphyrias with experiments to correct enzyme deficiency in tissues
Non-viral mediated gene transfers
-One study showed that active PBGD enzyme could be expressed in high levels in different cell systems by using non-viral gene delivery of plasmids (cDNA) into PBGD deficient cells (human and mouse). They supplied the cells with ALA and PBG and measured in increase in protoporphyrin (one of the porphyrins downstream in the pathway) in the PBGD defecient cells + plasmid with the enzyme.There have been some cases of liver transplantation in pts with severe porphyria with frequent disabling attacks ? one study of a 19 year-old women had a liver transplant with normalized urine porphyrin excretion and resolution of her acute attacks.
Animal models used to mimic porphyrias with experiments to correct enzyme deficiency in tissues
Non-viral mediated gene transfers
-One study showed that active PBGD enzyme could be expressed in high levels in different cell systems by using non-viral gene delivery of plasmids (cDNA) into PBGD deficient cells (human and mouse). They supplied the cells with ALA and PBG and measured in increase in protoporphyrin (one of the porphyrins downstream in the pathway) in the PBGD defecient cells + plasmid with the enzyme.
36. If You Were Asleep�.Key Points to Remember Porphyrias are metabolic diseases resulting from a partial deficiency of an enzyme in the heme biosynthetic pathway
Cause acute attacks secondary accumulation of heme precursors
Clinical features: abdominal pain, tachycardia, hypertension, hyponatremia, seizures, motor neuropathy etc.
Screen for porphyria with qualitative urinary PBG and if elevated measure quantitative urinary PBG and ALA
Confirm diagnosis with urinary and fecal fractionated porphyrins and DNA testing
Treat acute attacks with IV hemin
Prevent acute attacks with smoking cessation, avoidance of inciting agents
37. References Anderson, K. E. Recommendations for the Diagnosis and Treatment of the Acute Porphyrias. Annals of Internal Medicine. 2005; 142: 439-450.
Kauppinen, R. Porphyrias. Lancet. 2005; 365: 241-52.
James M.F. & Hift, R.J. Porphyrias. British Journal of Anaesthesia. 2000; 85: 143-53.
Sies, C. Clinical Indications for the Investigation of Porphyrias: Case Examples and Evolving Laboratory Approaches to its Diagnosis in New Zealand. The New Zealand Medical Journal. 2005; 118: 1-10.
Soonawalla, Z.F. Liver Transplantation as a Cure for Acute Intermittent Porphyria. The Lancet. 2004; 363: 705-6.
Onuki, J. Is 5-Aminolevulinic Acid Involved in the Hepatocellular Carcinotgenesis of Acute Intermittent Porphyria? Cellular and Molecular Biology. 2002: 48: 17-26.
Cimetidine and Acute Intermittent Porphyria
Floderus, Y. Variation in PBG and ALA Concentrations in Plasma and Urine from Asymptomatic Carriers of the Acute Intermittent Porphyria Gene with Increased Porphyrin Precursor Excretion. Clinical Chemistry. 2006; 52: 701-701.
Johansson, A. Correction of the Biochemical Defect in Porphobilinogen Deaminase Deficient Cells by Non-Viral Gene Delivery. Molecular and Cellular Biochemistry. 2003; 250: 65-71.
Andersson, C. Renal Symptomatology in Patients with Acute Intermittent Porphyria. Journal of Internal Medicine. 2000; 248: 319-325.
Bjersing, L. Hepatocellular Carcinoma in Patients from Northern Sweden with Acute Intermittent Porphyria: Morphology and Mutations. Cancer Epidemiology, Biomarkers, and Prevention. 1996; 5: 393-397.
Anderson, C. The epidemiology of Hepatocellular Carcinoma in Patients with Acute Intermittent Porpyria. Journal of Internal Medicine. 1996; 240: 195-201.
38. References De Siervi et al. Aminolevulinic acid cytotoxic effects on human hepatocarcinoma cell lines. BMC Cancer. 2002, 2: 1-6.
Seth, A. et al. Liver Transplantation for Porphyria: Who, When, and How? Liver Transplantation. 2007, 13: 1219-1227.
Bonkovsky, H. et al. Reconstitution of Hematin for Intravenous Infusion. Annals of Internal Medicine. 2006, 144: 537-538.
Siegert, S & Holt, R. Physicochemical Properties, Pharmacokinetics, and Pharmacodynamics of Intravenous Hematin: a Literature Review. Adv Ther. 2008; 25: 842-857.
www.porphyriafoundation.com/
40. The End