Download
1 / 54
540 likes | 690 Vues
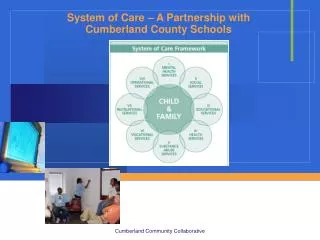
Integration of Schools and System of Care. IL Children’s Mental Health Partnership Conference June 26 – 27, 2012. Brief History – Systems of Care. 1969 – Joint Commission on Mental Health of Children – very few youth were receiving mental health services

E N D
Integration of Schools and System of Care IL Children’s Mental Health Partnership Conference June 26 – 27, 2012
Brief History – Systems of Care • 1969 – Joint Commission on Mental Health of Children – very few youth were receiving mental health services • 1982 – Jane Knitzer’s Unclaimed Children - youth were receiving services in overly restrictive settings • 1984 – Child and Adolescent Service System Program (CASSP) Model – first system of care • 1986 – System of Care approach & framework put forth by Stroul & Friedman • 1992 – Congress passed legislation for CCMHS – System of Care Grants
System of Care Communities of the Comprehensive Community Mental Health Services for Children and Their Families Program Funded Communities Date Number 1993–1994 22 1997–1998 23 1999–2000 22 2002–2004 29 2005–2006 30 2008 18 2009–2010 29
System of Care-Definition • “Spectrum of effective, community-based services and supports • For children and youth with or at risk for mental health or other challenges and their families • Organized into a coordinated network • Builds meaningful partnerships with families and youth • Addresses cultural and linguistic needs • Function better at home, in school, in the community and throughout life.” (SMHSA 2010)
Core Values Family Driven and Youth Guided • The strengths and needs of the child and family determine the types and mix of services • Families have primary decision-making role in ALL aspects concerning the care of their children
Community Based • Services and supports are provided within child and family’s community • Traditional as well as non-traditional • Informal service providers and supports are utilized
Culturally and Linguistically Competent • Organizations and programs reflect the cultural, racial, ethnic and linguistic differences of the populations they serve • Facilitates access to and utilization of services and supports • Eliminates disparities in care
Champaign County SOC JuliKartel & Jill Mathews-Johnson
Champaign County SOCACCESS Initiative Mission • Build a trauma and justice informed SOC • Designed to create a healed community • Works to ensure that youth and their families are resilient, resourceful, responsible and restored
Target Population • Youth 10-18 with social, emotional and behavioral challenges • Who are disproportionately represented in the juvenile justice and child welfare systems • and/or by negative academic and health outcomes
SPARCSStructured Psychotherapy for Adolescents Responding to Chronic Stress • Evidenced informed intervention • 16-one hour groups • Adolescents 12-21 • History of trauma (broadly defined) • Living with ongoing stressors • Exhibit functional impairment Structured Psychotherapy for Adolescents Responding to Chronic Stress (SPARCS) National Child Traumatic Stress Network www.NCTSN.org
Why SPARCS? • Was chosen by a committee of parents, youth and agency stakeholders • Had demonstrated positive outcomes for youth in foster care in Illinois • Broad definition of trauma fit for our community’s experiences • Flexible model allowed for youth input • Non-Master’s clinician can co-lead
Mental Health – School Collaboration Multiple Pre-planning Meetings • Introduce SPARCS to administrative team • Identification of appropriate students • Referral process • Consents/communication with parents • Protocols for student getting to/from group • Procedures for meeting w/ students individually
Identifying Students with Needs Data-based Decision Rules for Entrance • At Centennial High School: students were freshman or freshman status and • Through two tier two interventions and have not responded • Transitioning back from Regional Alternative School • Had multiple SASS contacts • Met criteria for trauma experience per TESI-SR(Traumatic Events Screening Inventory-Self Report)
Continued Meetings Mental health provider and PBIS T.A. Coordinator • Strengthen integration into PBIS Framework • Communication between school and community provider • Identification of school and mental health outcomes • Future planning for further tiered integration (skills only group)
Outcome Measures School (need to include data that we have) • ODRs • ISS/OSS • Grades/Credits • Attendance Mental Health • YOQ parent and youth • Youth group survey results SOC Evaluation • TRAC Noms • CANS • TESI
Organizational StructuresFunding • SAMHSA SOC Cooperative Agreement • United Way of Champaign County • Medicaid billing (future) • Probation/Court Services (future)
Feedback from Staff MH Staff: Positives • Being part of Tier II team helpful • Having school staff facilitate arrival/departures from group very helpful • Having one dedicated administrator is essential to coordination
Improvements Improvements • Protocols for communicating with mental health staff when crisis or disciplinary events occur • More time prior to group to get to know student and parent • Establish formal Collaborative Agreement
Feedback - Students • Student Survey Results 1=strongly agree 2=disagree 3= don’t know 4=agree 5=strongly agree Skills were helpful to me: • Mindfulness: 3.8 • Self-sooth/distract: 4.4 • LET ‘M GO: 4.0 • MAKE A LINK: 4.2 Have used skills outside of group4.4
Best Part of Group • “It helped me to make better choices and not get into trouble” • “That you can talk about stress level and feelings” • “It allowed me to share” • “It helped me to identify my sources of anger” • “I liked that it had structure, that we had a lesson plan that we followed and I liked the handbook” • “Food”
Future Goals • Identify incoming freshman – service Summer 2012 • Potential for multiple groups next year at Centennial; feeder middle school is also beginning 2012-2012SY • Refine data decisions for appropriate ID of students • Provide further teacher/staff training in SPARCS skills and develop plan for further integration of skills • Utilize students to co-lead group • Build stronger parent engagement • Build sustainability plan • Professional development plan for all staff
Systems Work Stakeholders
Collaborative Efforts • Schedule meetings with stakeholders • Bi-monthly “Secondary Systems” meetings • Monthly/Quarterly administrative meetings • Allows all stakeholders to have voice • Keeps communication lines open • Establish procedures and protocols • Create true partnerships • Stakeholders need to be seen as viable members in both settings (team membership, professional development) • Make interventions sustainable • Funding • Part of system of support
System of Care Framework, Philosophy and Outcomes Presented by: Angie Hampton, CEO
System of Care In 2009, EHD received the SAMHSA Children’s Mental Health Initiative grant for 6 years to transform our local children’s mental health system of care. Project Connect
SOC Guiding Principles • Comprehensive services • Broad array of services • Individualized to each child and family • Provided in the least restrictive environment • Coordinated at both the system and service delivery levels • Organized to include families and youth as full partners • Designed to emphasize early identification and intervention
SYSTEM OF CARE • The System of Care approach can provide both a conceptual framework and specific strategies for implementation of the ACA in ways that ensure that the behavioral health needs of children, adolescents, young adults, and their families will be effectively. • The System of Care approach has been the major framework for improving delivery systems, services, and outcomes for children with mental health needs for the past 25 years, shaping system reforms in many states.
SYSTEM OF CARE • Extensive research and evaluation have documented the effectiveness of this approach for improving the organization and delivery of children’s mental health services, and for improving clinical and functional outcomes for children and their families.
Integrated Care • EHD is integrating services with a local FQHC. • A Care Coordinator is being hired by EHD but located in the FQHC. (co-location) • Illinois DocAssist contract (behavioral health consultation to primary care providers in Region V) • A Family Nurse Practitioner is on staff to provide Medical Home services to complex cases as well as provide behavioral health consultation services to primary care providers
Health Homes • The health home concept is closely aligned with the system of care approach, sharing many of the same values and operational principles. • The major goal of the health home model is to provide more comprehensive, coordinated, and cost-effective care for individuals with disabilities than is generally provided when services are fragmented across multiple health providers and organizations. Designed to operate under a “whole-person approach”
Health Homes • System of Care approach can serve as a model for implementation of health homes- not only for children with behavioral health disorders, but for other health care populations as well.
System of Care=Health Reform • Systems of care and health reform are both designed to: • Increase access to health care services • Increase the array of available services and supports • Improve the coordination of care • Improve the quality and outcomes of care • Improve the cost-effectiveness of services, and • Better invest resources.
Systems of Care=Health Reform • Systems of care have demonstrated that the availability of a broad range of treatment and support services for children’s behavioral health is effective in preventing more serious problems and mitigating overall health care system costs. • An individualized, wraparound approach to service planning and delivery has proven effective and ensures that children and their families receive optimal, appropriate, and cost-effective care.
Systems of Care=Health Reform • Care coordination and management at the individual and system levels have reduced fragmentation and resulted in better use of resources. • Systems of care have demonstrated that there are cost-reducing and cost-effective alternatives to serving children in hospitals, residential treatment centers, and other institutional settings.
Youth in Transition to Adulthood Presented by: Liz Doyle, Clinical Director and Sharon Slover, Director of Education & Careers, McHenry County Family CARE System of Care Grant 2006 - 2012
Statement of the Problem • U. S.: 3,000,000 transition youth have serious emotional disorders - APA Fact Sheet (2000) • Prevalence is greatest among 18 – 25 year olds (12%) of population • 60% of TY with SED do not complete high school, 3 Xs greater risk for JJ involvement, & higher risk for substance abuse
Transitional Youth in State of IL • 1,617,703 (age 16 – 24) (2010 census) • 12 % with serious emotional dx = 194,124 • ISBE Stats (2010): 58,544 with IEPs (age 16+); 101, 079 with IEPs (age 14+)
Identification of Transitional Youth in McHenry County through Family CARE • 10/2005 – Received SAMHSA System of Care cooperative agreement for 6 years • TY - one of 4 populations of focus • McHenry County (2010): 33,779 TY (age 16 – 24); estimated 4,053 (12%) with SED • Youth in Special Ed: 3,621 (age 12 – 21) • Youth receiving MH services: 1,200 (age 16 – 24)
Using System Of Care Principles to Identify and Meet Needs of TY • TYWG and Youth Council • Development of Youth Voice • Choosing an EBP: Identification of Transition to Independence Process (TIP) Model by Youth and Parents
TIP Process • Engage young people • Tailor services and supports • Develop personal choice • Ensure a safety net of support • Enhance young persons’ competencies • Maintain an outcome focus • Involve young people, parents, and other community partners
Needs of Transitional Youth • Youth Needs: Life Skills and Education • Training Needs in EBP • Adolescent & Adult; School and MH • Shared training – use of same language • Lack of Coordination • Lack of Specialized Programming
Transition to Adulthood Program (TAP) • Youth-Guided Process • Home-Based Case Management Program • Strengths-based and futures planning • Fidelity to the TIP Process • Specialized Programming for TY • Development of Formal and Informal Supports