Download

1 / 46
460 likes | 720 Vues
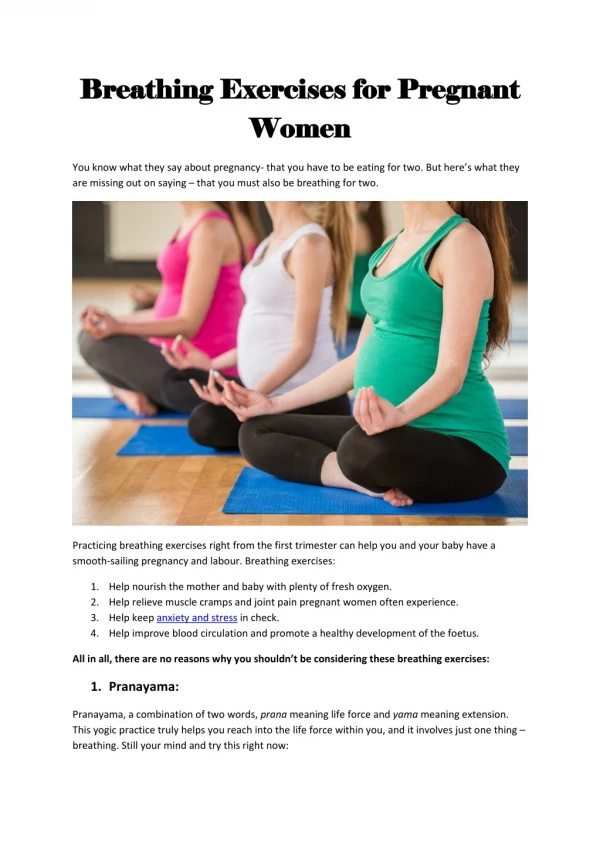
Sleep Disordered Breathing in Pregnant Women. By Prof. Suzan Salama Professor of Pulmonology and Sleep Medicine Assiut University. Adaptation of the circulation:. Physiology of pregnancy. Adaptation of the respiratory system. Typical arterial blood gases values.

E N D
Sleep Disordered Breathing in Pregnant Women By Prof. Suzan Salama Professor of Pulmonology and Sleep Medicine Assiut University
Adaptation of the circulation: Physiology of pregnancy
Sleep disordered breathing in non-pregnant women 1- OSA 2- Upper airway resistance 3- Central apnea • The OSA is a frequent but often unrecognized condition, especially in younger women. • Wisconsin sleep cohort study recorded.
Ninety three (93%) of women with moderate to severe OSA were not clinically diagnosed in the Wisconsin study. • Under-diagnosis was most frequently encountered among women, younger, poorer, less educated and who had not yet developed hypertension or atherosclerotic disorder.
Burden of OSA • Burden of the disease: In comparison to persons without OSA • The presence of moderate to severe OSA was associated with: (1)Hypertension with an (odd ratio of 2.9) at 4 years follow up especially at age (40-59 years). (2) The presence of mild OSA (AHI >5) was an independent risk factor for prevalent coronary disease (odds ratio 4.1).
(4) OSA is an independent risk factor for incident strokes. (5) OSA is an independent risk factor for incident atrial fibrillation. (6) OSA is associated with prevalent congestive heart failure. (7) OSA is associated with prevalent glucose intolerance and insulin resistance. (8) Oxygen desaturation index (>4%) is a better predictor of insulin resistance than BMI.
Clinical presentations of OSA in women The classic OSA presentation that is: • Older obese men, with loud and habitual snoring. • Witnessed apneas and EDS. Women with OSA were differ with men matched as regards age, AHI, BMI and Epworth sleepiness score complaining with: • Frequent insomnia. • Nocturnal palpitation. • Depression • Hypothyrodism. • Asthma and allergies. • Migraine. • Weakness, drowsiness, lack of energy. • Irritable bowel syndrome.
Don’t focused On the classic OSA presentations
Risk factors of OSA in women • Age: • The prevalence among women 30-39 years (10.9%). • 6.5% mild OSA (AHI >5). • 4.4% moderate severe (AHI >15). • The prevalence among pre-menopausal (40-55) years old (14.4%). • 10.8% mild OSA. • 3.6% moderate to severe OSA.
(2) Obesity: • A well-demonstrated risk factor of OSA. World health organization (WHO) defines obesity among Indian women as: • BMI >25kg/m2. • Waist-hip ratio > 0.8. • Neck circumference >43cm. • Waist circumferences > 88cm. • Skin hold thickens. • Obesity a risk factor for 41% of the mild OSA 58% of moderate to severe OSA. • World wide obesity epidemic in 25% of men in 36% of women.
(3) Craniofacial features: Associated with narrowed upper airway (long-narrow face, large tonsils) among far east Asians odds ratio 2.51. (4) Chronic rhinitis, asthma: A strong marker for OSA (odds ratio 3.2). (5) Polycystic ovarian syndrome: The prevelance of OSA among women with polycystic ovarian syndrome as high as 70%.
(6) Menopause: Is associated with 2.6 odds ratio of having OSA (AHI >5), adjusted for age, BMI, smoking, exercise, alcohol, cardiovascular disease. (7) Pregnancy: Is a risk factor for snoring and OSA in obese women.
(1) Alterations of sleep in normal pregnancy 1- Changes in the sleep pattern and architecture. During the first trimester: • Increased: • Sleep duration, daytime sleepiness, • Insomnia, sleep disturbances. • PSG: • Increased total sleep time. • Decrease of: - Sleep efficiency. - Stages 3 and 4 and REM sleep.
In the second trimester: - Normal nocturnal sleep times. - Increase sleep complaints (nocturia, fetal mov.). • PSG:- Reduced (stages 3 and 4). - Reduced (REM). In the third trimester - Decreased total sleep time. • PSG - Increase stage 1 and 2. - Decrease stage 3, 4 and REM stages.
Sleep disorder breathing in pregnancy • Although during pregnancy in normal women oxygen desaturation is reduced in the supine position. • Mild respiratory disturbances during sleep in late pregnancy may result in significant reduction of maternal and fetal oxygenation. • After delivery nocturnal oxygenation return to normal. • Severe OSA, that was significantly improved 12 weeks postpartum.
Promoting mechanisms of SDB Physical changes: A- The elevation of the diaphragm results in: • Reduction of functional residual capacity • Maternal oxygenation reserve is reduced because of increased alveolar-arterial oxygen gradient. • Ventilation-perfusion mismatch, due to closure of airway above FRV during tidal ventilation. (Prominent in late pregnancy and in the supine position).
B- The increase of blood volume during pregnancy resulting in hyperemia and edema of nasal mucosa. C- High estrogen level, may cause vasomotor rhinitis in 20%-42% in the third trimester and reduced nasopharyngeal patency.
(2) Hormonal changes: A- High circulating levels of progesterone and estrogen: • Enhance respiratory drive resulting in hyperventilation. • Leads to a reduction of arterial carbon dioxide pressure PaCO2 28-32. • Respiratory alkalosis pH= 7.47. • Increased the frequency of central apneas. • The enhanced respiratory drive, lead to more negative inspiratory pressures, increased suction pressure on (UA) upper airway structures, and a tendency for collapse of (UA) during sleep.
Protective mechanisms of SDB 1- Physical changes: • Supine sleep posture increase the frequency of OSA events compared with lateral or prone positions. • Lateral position preserves cardiac output and oxygenation. • The observed reduction of REM sleep during late pregnancy may protect pregnant women from SDB.
2- Hormonal changes: • Increase minute ventilation, may serve as an adaptation to the increased oxygen consumption demands of pregnancy. • Progesterone stimulates respiratory drive, resulting in increased tidal volume and hyperventilation. • The higher respiratory drive, enhances responsiveness of upper airway dilator ms to chemical stimuli. • Progesterone increases the electromyographic activity of pharyngeal dilating muscles, to protect against SDB.
Risk factors for OSA during pregnancy (1) Snoring • There is evidence that snoring is increased during pregnancy and is common in the third trimester in 27%. • Self reported snoring recorded 14% of 350 pregnant women of the second trimester. • There is reduction of snoring at 5% at 3 months after delivery. • Not only snoring but also gasping, choking and witnessed apneas were increased significantly during pregnancy.
(2) Obesity • Obesity is a major risk factor for sleep apnea generally. • During pregnancy, increased initial body mass index and greater changes in neck circumference have been associated with higher prevalence of SDB. • Habitual snoring associated with weight gain. • Neck circumference is a predictor of sleep apnea, independent of weight, which reflect the changes in the upper airway anatomy.
During pregnancy Maternal Complications Due to SDB
Maternal complications due to SDB (1)Preeclampsia: is condition that may complicate 5% to 6% of pregnancies characterized by PIH (pregnancy included hypertension) and proteinurea (>300mg/d) that may result in maternal morbidity and mortality, premature delivery and fetal growth retardation. Known risk factors for preeclampsia include: • Family history primiparity. • Advanced maternal age – obesity. • Pre-existing hypertension – renal disease.
Mechanism of link (preeclampsia and OSA): • The pathogenesis of preeclampsia is not known but, recently it has been associated with oxidative stress and endothelial dysfunction. • OSA is common in the general population ad has been linked with the development of arterial hypertension even in cases of mild severity.
Moreover, it has been hypothesized that OSA and nocturnal hypoxemia activate the sympathetic nervous system, impaired endothelial function, elevate the levels of vasoconstriction substances, and cause the development of oxidative stress leading to inflammatory changes and vascular damage. • Hypoxemia and increased body weight during pregnancy may occur without the presence of significant SDB, however, and may predispose to the development of PIH.
Absence of nocturnal dipping (10-20mmHg) in systolic blood pressure is seen in both preeclampsia and OSA, suggesting a common link between the two. • In a study showed that preeclampstic women had significantly higher RDI (18.4vs 8.3; P<0.05). And lower endothelial function index (1.5 vs 1.8; P<0.05); compared with the control group.
Results in: • Reduced oxygen placental delivery to the fetus. • These mechanisms suggest a relationship of sleep apnea with intrauterine growth retardation and small birth weight. • Several studies report the presence of OSA syndrome in pregnant women associated with: - PIH and preeclampisa. Or - Pulmonary hypertension. Or - Gestational diabetes.
Evaluation and screening of OSA during pregnancy 1- There are no specific guidelines for screening pregnant women for OSA. 2- Pien and Schwab (2004), have proposed that pregnant women with. • ED sleepiness. - Loud snoring. • Witnessed apnea. - Preexisting obesity. • Large neck size with PLM. • Preeclampsia should be evaluated for OSA with overnight PSG.
3- Santiago et al., (2001) argued that until the incidence of SDB in normal and complicated pregnancy is defined, the indications of PSG should be expended to include those with: • Hypertension. • Previous babies with unexplained intrauterine growth restriction. • Persistant sleep-related symptoms (hypersomnia or insomnia). • Associated with snoring or obesity Strength of recommendation, C.
There are multiple studies that have successfully performed nocturnal PSG without difficulty. • However, the preference of pregnant women to sleep in the lateral position, it is possible that AHI may be under estimated.
Fetal complications: • Intermittent hypoxia during pregnancy observed with OSA, leads to placental ischemia, causes fetal heart rate decelerations, decreased fetal breathing and movements and fetal growth restriction. • Franklin et al., (2000), found that pregnant women with self reported snoring delivered infants with lower APGAR scores and lower weight (7.1vs 2.6) than non snorers.
SDB had been proposed as a risk factor for adverse fetal outcomes: • Fetal heart rate abnormalities. • Fetal growth retardation. • Fetal death. • On the other hand, a study on 325 pregnant women did not find relationship between snoring and infant birth weight.
Treatment of OSA during pregnancy • Conservative measures: • Control of body weight gain. • Avoidance of sleep in the supine position. • Elevation of the head during sleep. • Restriction of alcohol and sedatives consumption. • These measures are useful even in non-OSA pregnant women (strength recommendation, C).
(2) Nasal CPAP: • CPAP is the therapy of choice for OSA. • CPAP during pregnancy has been shown to be safe, effective and well tolerated. • CPAP is not recommended in preeclampsia without objective documentation of OSA (strength recommended, A). • CPAP recommended in pregnant women with (mild apnea AHI>5-30 events/h), and severe apnea (AHI >30 events/hour) or recurrent SaO2 <90%. • CPAP therapy also has been shown to improve cardiac output while reducing total peripheral resistance in patients with preeclampsia.
(3) Oral appliances: • Have not been investigated and impractical. (4) Surgical therapies: (uvulopalatopharynegeoplasty). • Are not recommended during pregnancy, because they are less effective.
(5) Oxygen therapy: • For pregnant women who refuse to use or are unable to tolerate CPAP, to improve minimal oxyhemoglobin saturation. • No recommendation for chronic use of oxygen as a therapy for OSA as a primary treatment. • Moreover, there are potential dangers like prolongation of apnea duration, increased hypercarbia, and ventricular irritability associated with oxygen therapy.
Post partum management of OSA • OSA precipitated by pregnancy usually improves after delivery. • Significant spontaneous improvement of AHI values, SaO2, arousal indices occurred by 3 to 6 months postpartum. • Nasal CPAP was discontinued within 2 weeks of delivery in all the patients.
Based on expert opinion (2004): 1- Postpartum withdrawal of CPAP therapy with follow up in mild to moderate OSApregnancy associated for symptoms recur, a repeat PSG to assess baseline AHI is indicated. 2- For severe pregnancy-associated sleep apnea, therapy should be continued and, when weight returns to 10% to 15% of baseline, repeat PSG to establish baseline, of AHI and any need for continued therapy.
patients with pre-existing OSA can safely, when their weight returns to 10% to 15% of baseline, repeat PSG to determine new AIH. • All women with gestational sleep apnea should monitored closely for symptoms recurrence in subsequent pregnancies.