Download
1 / 29
290 likes | 645 Vues
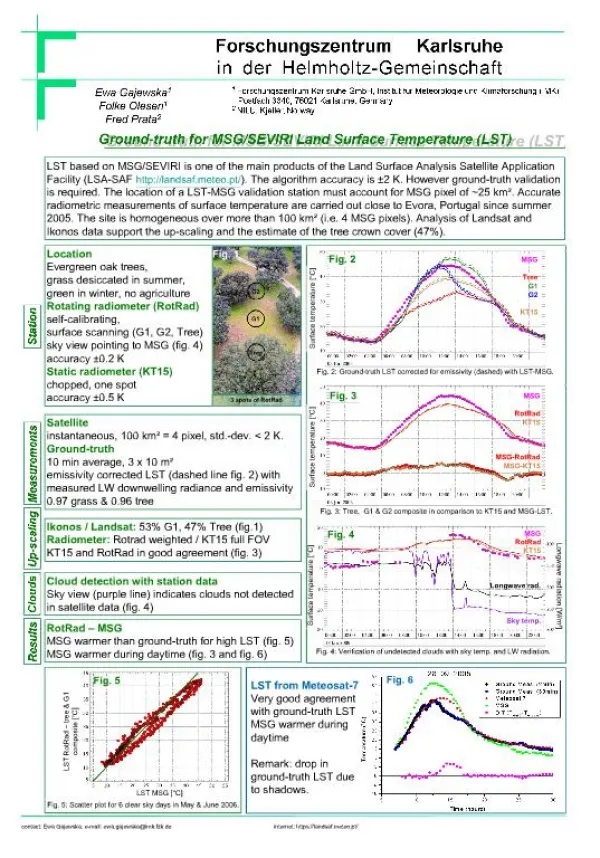
The potential role of human papillomavirus (HPV) infection in vertical HIV transmission: HPV co-infection in subtype C HIV-1-infected pregnant women in Zimbabwe. David Hill, PhD Stanford University 25 September 2006. HPV: what is it?.

E N D
The potential role of human papillomavirus (HPV) infection in vertical HIV transmission:HPV co-infection in subtype C HIV-1-infected pregnant women in Zimbabwe David Hill, PhD Stanford University 25 September 2006
HPV: what is it? • a DNA virus that causes epithelial proliferations at cutaneous and mucosal surfaces • 106 genotypes have been identified (likely ~100 more); >30 infect anogenital epithelium • HPV is transmitted by skin-to-skin contact • Biggest single risk factor: high # of sexual partners
HPV: what is it? • Genital infection with HPV is the world’s most common STI; ~80% of sexually active people are infected at some point in life • Most HPV infection is transient, asymptomatic, resolves w/o treatment • 70% clear within 1 year; >90% clear within 2 years • Median duration of new infection: ~8 months • Persistent infection with high-risk types causes almost all (99%+) cervical cancer
High-risk types Associated with invasive cancers(esp. cervical) common types: 16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 68, 82 Low-risk types Cause low-grade cell changes and genital warts common types: 6, 11, 40, 42, 43 44, 54, 61, 72, 73, 81 HPV: what’s ‘high-risk’?
HPV and cervical cancer • HPV infection peaks in young women (early sexual activity) • Cervical cancer typically follows 20-30 years later • Cervical cancer affects 0.5 – 1.5 million women per year • Kills nearly 0.25 million per year • 80% of cervical cancer cases are in the developing world • Major health inequity • Highest incidence: sub-Saharan Africa & Latin America • Prevention: regular gyn screening (pap) & treatment of precancerous lesions
HPV vaccines • June 2006: the US FDA licensed Merck’s Gardasil • quadrivalent, protects against 6, 11, 16, 18 • Trials showed: safe, good immune response, efficacious • Guards against 70% of cervical cancers and 90% of genital warts • Later in June ’06: the Advisory Committee on Immunization Practices (ACIP) recommended routine vaccination for girls 11-12 years; also made vaccine available to 9-26 year olds.
HPV vaccines • GSK vaccine (still in phase III) • bivalent, protects against types 16 & 18 • Why not develop a vaccine with 7 types? Technical hurdles are many • Mathematical models indicate that these vaccines (vs. 16 & 18) will reduce an individual’s lifetime risk of developing cervical cancer by ~50% (no ref)
HPV: purpose of our study • To define prevalence and types of HPV in HIV-1-infected pregnant women in urban Zimbabwe • HPV prevalence reported elsewhere: • ~30% in (sexually active) general population • Estimated worldwide prevalence of 400-500 million • Little geographic variation • ~60% among HIV-infected women 2. To pilot an investigation of the association of HPV infection with MTCT • Based on our knowledge of other sexually transmitted infections (STIs), and their role in facilitating HIV transmission
Rationale for our study • Much evidence of STIs amplifying HIV transmission • Non-ulceratives: inflammation, increaselocal presence of targeted cells • Ulcerative STIs: provide portals of entry • Presence may increase amount of virus shed in genital tract • STIs in the context of HIV has generally not included HPV • HPV *should* be considered b/c of this potential influence on immune response & physical lesions • Our hypothesis is that HPV in genital tract will increase HIV shedding & may facilitate HIV transmission to infants • Understanding this relationship may help us develop more comprehensive treatment & prevention strategies
Global HIV and AIDS statistics by region, end of 2005 N (%) UNAIDS, World Health Organization
North America 9 000 [0.4%] Sub-Saharan Africa 2.1 mill. [91%] Total: 2.3 (2.1 – 2.8) million Children (<15 years) estimated to be living with HIV end 2005 N [%] Total children living with HIV: 2.3 million UNAIDS, World Health Organization
North America 9 000 [0.4%] 100 [0.02%] Sub-Saharan Africa 2.1 mill. [91%] 520,000 [91%] Total: 2.3 (2.1 – 2.8) million Children (<15 years) estimated to be living with HIV, and dying of AIDS end 2005 N [%] Total children living with HIV: 2.3 million Total children dying of AIDS: 570,000 UNAIDS, World Health Organization
Features of perinatal HIV/AIDS: a “tale of two epidemics” LM Newell et al, Lancet 2004; 364 and L Mofenson
Research in PMTCT of HIV1994 EM Connor et al, NEJM 1994;331
Incident pediatric AIDS Cases in the U.S.acquired via perinatal HIV, 1985-1999 Number of Cases Quarter-Year CDC
Five antiretroviral therapy (ART) trials for PMTCT1999-2003 Dabis 1999; Wiktor 1999; Saba 2002; Jackson 2003; Moodley 2003; pooled analysis in Leroy AIDS 2005
Maternal characteristics, by HPV status (N=57) No statistically significant differences were identified across groups in any category
Prevalence of maternal HPV, by infant HIV status
Prevalence of HPV by high and low risk groups in all mothers and in groups of infant HIV status *Subgroups of subjects (by phylogenetic category) were not mutually exclusive. a 53, 56, 66 b 18, 26, 45, 59, 68, 69, 70 c 16, 31, 33, 52, 58 d 6, 11, 40, 54, 55 e 61, 73, AE2, Pap 155, Pap 291, generic probe positive only
Prevalence of HPV by high and low risk groups in all mothers and in groups of infant HIV status *Subgroups of subjects (by phylogenetic category) were not mutually exclusive. a 53, 56, 66 b 18, 26, 45, 59, 68, 69, 70 c 16, 31, 33, 52, 58 d 6, 11, 40, 54, 55 e 61, 73, AE2, Pap 155, Pap 291, generic probe positive only
Logistic regression models: Risk of vertical HIV transmission in HPV-positive and HPV-negative mothers (adjusted for baseline maternal CD4+ cell count) a OR, odds ratio; CI, confidence interval b 2-tailed P value c High-risk HPV: any 16-like, 18-like, or 56-like HPV d Low-risk HPV types: 2, 6, 11, 13 , 32, 40, 42, 44, 54, 55, 57, 62, 72 e Other HPV types: 61, AE2, Pap155, Pap291, 73, mixture, or consensus probe positive only
Conclusions • A high proportion of HIV-infected pregnant women in this population have cervical HPV infection • A broad diversity of HPV types is present • There is a high prevalence of HPV types associated with increased risk of cervical cancer • This preliminary assessment of HPV carriage warrants further study of • HPV types • HIV cervical shedding • the association between HPV and MTCT of subtype C HIV-1
David Katzenstein Bonnie Maldonado Julie Parsonnet Richard Roberts Kristin Cobb Avinash Shetty Catherine Ley Joel Palefsky Patrick Mateta Lynn Zijenah Acknowledgments
Developing, resource-poor Economic barriers Lack of infrastructure Lack of money Lack of people Social, cultural barriers Stigma Government barriers Lack of political will Industrialized, resource-rich Funding available Stable infrastructures Someone pays Robust health system Fewer social barriers Advocacy Governments act Advocacy Factors affecting perinatal HIV: worlds apart