Download
1 / 31
310 likes | 541 Vues
C4d in pancreas transplant biopsies: the Leiden experience Ingeborg Bajema Ingeborg Bajema. Ingeborg Bajema. Introduction. Taking biopsies from pancreas transplants was uncommon until the early 1990s when a technique of percutaneous needle biopsy was introduced

E N D
C4d in pancreas transplant biopsies:the Leiden experienceIngeborg BajemaIngeborg Bajema Ingeborg Bajema
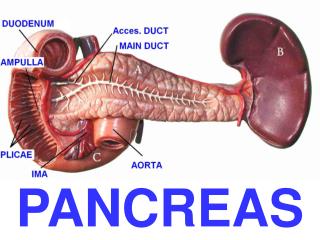
Introduction • Taking biopsies from pancreas transplants was uncommon until the early 1990s when a technique of percutaneous needle biopsy was introduced • Each year, circa 3000 pancreas transplants are performed worldwide, 75% in the setting of a SPKT, mostly for patients with diabetes type 1 • Some hospitals follow serum creatinine as a surrogate markers for pancreas rejection
Pancreas rejection: Drachenberg et al, Am J Transpl 2008 Working proposal for grading pancreas allograft rejection • Normal • Indeterminate • Cell-mediated rejection (grade I, II, III) • Antibody-mediated rejection • Chronic allograft rejection/graft sclerosis • Other histological diagnosis (e.g. CMV pancreatitis, PTLD)
Pancreas rejection: Drachenberg et al, Am J Transpl 2008 Working proposal for grading pancreas allograft rejection • Normal • Indeterminate • Cell-mediated rejection (grade I, II, III) • Antibody-mediated rejection • Chronic allograft rejection/graft sclerosis • Other histological diagnosis (e.g. CMV pancreatitis, PTLD) • The role of a C4d staining in relation to AMR is only beginning to be described
Pancreas rejection: Drachenberg et al, Am J Transpl 2008 Working proposal for grading pancreas allograft rejection Antibody-mediated rejection: • Complement deposition in vessels (i.e. capillary C4d deposition) which can be accompanied by monocyte/macrophage and neutrophil margination within interstitial capillaries • Graft dysfunction • Donor-specific antibodies (DSA) in serum
Overview of literature: Melcher, Am J Transplant, 2006 Melcher in 2006 were the first to report a patient with a SPKT who developed AMR with donor-specific HLA-DR allo-antibodies and had positive C4d staining in the pancreas one month after a SPKT. The renal transplant biopsy of this patient taken at day 10 was also positive for C4d. pancreas kidney
Overview of literature: Carbajal et al, NDT 2007 Carbajal et al a year later reported a patient with pancreas after kidney transplantation (PAK) who developed AMR of the pancreas with C4d positivity in the biopsy. The kidney, which was from a different donor, remained unaffected, but the pancreas graft was lost
Overview of literature: Gaber, Arch Pathol Lab Med 2007 Gaber reported one case of a C4d positive surveillance biopsy taken 2 weeks after transplantation from a patient who was sensitized by two previous islet transplants and had detectable anti-HLA antibodies
Overview of literature: Pascual, JASN 2008 Pascual reported 13 patients with an acute rejection of the pancreas of which 2 were biopsy-proven, and these were positive for C4d staining. In one patient, two biopsies of the pancreas were taken. DSA were negative at the time of the first biopsy, which was C4d positive. Three months later, a second biopsy was taken which was C4d positive as well, and by that time DSA were also positive
Overview of literature: Torrealba et al, Transplantation 2008 Torrealba et al reported on the potential role of C4d in pancreas transplant biopsies with AMR in a group of 18 patients 27 biopsies from 18 patients Correlation between C4d+, development of DSA and graft dysfunction There is potential value of C4d staining in the diagnosis of AMR of pancreas allografts
Overview of literature: comment by Munivenkatappa et al. to Torrealba et al, Transplantation 2009 C4d+ can be encountered in various clinical settings: 2/4 patients with C4d+ had typical AMR In one patient, C4d+ was associated with recurrent diabetes Another patient (with circulating DSA), remained euglycemic after 12 months of follow-up and without treatment of AMR
Overview of literature: reply from Torrealba et al. To comment by Munivenkatappa et al., Transplantation 2009 …. there is perhaps a spectrum of clinical scenarios, tissue evidence of antibody activation, and serologic patterns that still need to be defned to better understand AMR as an entity in pancreas allograft.
Whole pancreas transplantation at LUMC • 109 pancreas transplants between 1991 – 2001 • All SPKT • Pancreas transplant biopsies were taken on clinical indication until 2001 • 19 biopsies from pancreas transplants in this study • 26 pre-transplant biopsies
Pancreas transplant biopsies from LUMC • 19 biopsies from 18 patients • 17/19 biopsies taken because of clinically suspected rejection • 10 renal biopsies taken at the same time • H&E slides scored according to BANFF working proposal • C4d immunostaining was performed on 4 μm paraffin sections • C4d positivity: • Diffuse: > 50% of interacinar capillaries positive staining • Focal: 5 to 50% of interacinar capillaries positive staining • Minimal: < 5% of interacinar capillaries positive staining • Of 13/18 patients, DSA assessment was available
C4d staining patterns negative diffusely + focally +
Recipient characteristics • Mean age: 38.9 years (SD: 8.3) • Gender, % male: 67% • Years of DM1 at Tx: 6.9 years • % of women pregnant before Tx: 67% • Biopsy taken at day (mean, range): 97 (12-481) • DSA: negative in 6, positive in 7
Results 2 / 24 pre-transplant biopsies showed diffuse C4d staining pattern
Results Rest (83%) > 5yr graft survival R=rejection o=no rejection n =negative F=focal positive D=diffuse positive
Results Rest (83%) > 5yr graft survival R=rejection o=no rejection n =negative F=focal positive D=diffuse positive
Results Rest (83%) > 5yr graft survival R=rejection o=no rejection n =negative F=focal positive D=diffuse positive
Results Rest (83%) > 5yr graft survival R=rejection o=no rejection n =negative F=focal positive D=diffuse positive
Results Rest (83%) > 5yr graft survival R=rejection o=no rejection n =negative F=focal positive D=diffuse positive
C4d staining in simultaneous pancreas and kidney biopsies (case 8) focally +
A cooperation between LUMC and UMMC • UMMC: • 148 pancreas transplantations between 2000 and 2007 • 37 pancreas transplant biopsies, taken on clinical indication
AMR and graft survival 27 patients with C4d and DSA results available were categorized into 3 groups: I: minimal or no C4d staining, no DSA (N=13) II: diffuse C4d staining, no DSA (N=2); focal C4d staining and DSA (N=2); minimal/no C4d staining and DSA (2) III: Diffuse C4d staining and DSA (N=9)
Conclusion • C4d+ in the pancreas is independent of Banff classification • C4d staining patterns can differ per organ (kidney/pancreas) • C4d positivity alone, has no effect on pancreas survival • 1 patient DSA, Banff and C4d positive pancreas lost
Conclusions • Diffuse C4d positivity with concurrent DSA had poor graft survival, most likely related to AMR • Patients did well who had: • either DSA or C4d alone • or no DSA or C4d • The sole occurrence of either C4d or DSA poses no additional risk for poor outcome of the pancreas graft
Conclusions The results from our study emphasize the importance of taking into account a combination of C4d staining pattern, histological diagnosis and presence of DSA before a diagnosis of AMR of the pancreas is made
Acknowledgements Univ. of Maryland, School of Medicine, Baltimore, USA Department of Pathology Raghava Munivenkatappa Cinthia Drachenberg Benjamin Philosophe All doctors who contributed patients LUMC, the Netherlands Department of Pathology Hanneke de Kort Jan A. Bruijn Emile de Heer Department of Nephrology Eelco de Koning Cees van Kooten Stefan Berger Department of ImmunoHematology and Blood Transfusion (IHB) Michael Eikmans