Download
1 / 1
10 likes | 169 Vues
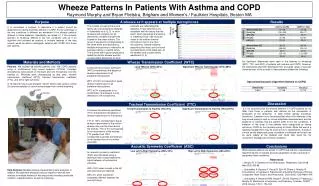
Wheeze Patterns In Patients With Asthma and COPD Raymond Murphy and Bryan Flietstra, Brigham and Women’s / Faulkner Hospitals, Boston MA. Purpose. A wheeze as it appears at multiple microphones. Results.

E N D
Wheeze Patterns In Patients With Asthma and COPDRaymond Murphy and Bryan Flietstra, Brigham and Women’s / Faulkner Hospitals, Boston MA Purpose A wheeze as it appears at multiple microphones Results The concept of a abnormal sound family was introduced and validated in Vyshedskiy et al (2, 3). In short, wheezes and crackles can be detected by multiple microphones located on the chest surface. The group of waveforms corresponding to the same event and recorded by multiple microphones is referred to as a wheeze family or crackle family. The channel with highest amplitude is called the mother wheeze and the corresponding deflections at other channels are called daughter wheezes. These definitions are consistent with the theory that the event, which generated a wheezing or crackling sound, had occurred closer to the mother channel microphone than to the other microphones. Indeed evidence supporting this theory can be found by examination of the stack plots of the wheeze and crackles family waveforms (2, 3). Wheeze family It is sometimes a problem to determine if a patient should be diagnosed as having bronchial asthma or COPD. As the pathology of the two conditions is different we wondered if the wheeze patterns differed in these diseases. Specifically we asked (1) if the acoustic features of wheezing differed in the two conditions and (2) if an algorithm that included an analysis of multiple features of the lung sounds would be able to distinguish patients with COPD from those with asthma. Materials and Methods Wheeze Transmission Coefficient (WTC) No significant differences were seen in the features of wheezing (WTC, TTC, and ASC) of patients with asthma and COPD. However, the specialized algorithm developed from a broader range of acoustic characteristics of the sounds in these patients yielded the following: Specialized Acoustic Algorithm (Asthma vs COPD) Patients: We studied 66 asthma patients and 109 COPD patients using a multichannel lung sound analyzer (STG16). Fourteen microphones were placed on the back and one microphone over the trachea (1). Wheezes were characterized by rate, pitch, wheeze transmission coefficient (WTC), tracheal transmission coefficient (TTC), and left to right symmetry. A 16-channel lung sound analyzer (shown below) was used to collect 20 seconds samples of sound during deeper than normal breathing. Local Wheeze (WTC=32%) Significant Wheeze Transmission (WTC=59%) A wheeze transmission coefficient (WTC) characterizes the degree of wheeze transmission to all ipsilateral microphones.WTC of 100% corresponds to equal wheeze transmission to all ipsilateral microphones. WTC of 0% corresponds to no transmission (the wheeze is only detected in one microphone). Discussion Tracheal Transmission Coefficient (TTC) Conclusions It is not surprising that the wheeze patterns in COPD patients do not differ from those in patients with asthma as the mechanism of production of the wheezing is likely similar (airway narrowing, secretions). Likewise it is not surprising that when other features of the lung sound patterns such as sound amplitude measurements and the presence of crackles that the pattern differ in the two conditions. A limitation of the study is that patients were categorized as having asthma or COPD by the clinicians caring for them. While this was at a teaching hospital there may be some errors in classification. A study of a more strictly diagnosed group of patients is indicated as the test can be done readily at the bedside and could help avoid the not uncommon misdiagnosis of these conditions. Trivial Transmission to Trachea (TTC=5%) Significant Transmission to Trachea (TTC=261%) A tracheal transmission coefficient (TTC) characterizes the degree of wheeze transmission to the trachea. TTC of 100% corresponds to equal wheeze transmission to the mother wheeze site over the chest and to the trachea. TTC of 0% corresponds to no transmission to the trachea. TTC greater than 100% corresponds to greater transmission to the trachea than to the mother chest site. Acoustic Symmetry Coefficient (ASC) While wheeze patterns are similar in COPD and asthma, a specialized algorithm based on multiple acoustic parameters shows a promise of separating these conditions. References Low Left to Right Symmetry (ASC=18%) High Left to Right Symmetry (ASC=55%) An acousticsymmetry coefficient (ASC) was calculated using a technique that crosscorrelated the signal between all symmetrical channels.ASC=100% when sounds in the left and right lungs are identical. ASC=0% when sounds are completely different between left and right lungs. • Murphy R. In Defense of the Stethoscope. Respiratory Care 2008 Mar;53(3):355-69 • Vyshedskiy A, Bezares F, Paciej R, Ebril M, Shane J, Murphy R. Transmission of Crackles in Patients with Interstitial Pulmonary Fibrosis, Congestive Heart Failure, and Pneumonia. Chest 2005; 128:1468-1474; • VyshedskiyA, AlhashemRM, PaciejR, EbrilM, RudmanI,FredbergJJ, MurphyR. Mechanism of Inspiratory and Expiratory Crackles. CHEST 2009 January 135(1): 156-164 Data Analysis: Multiple wheeze characteristics were analyzed. In addition the data were analyzed using an algorithm derived from analysis of multiple features of the lung sounds including amplitude variation, crackle features, as well as wheezing.