Download
1 / 81
820 likes | 1.25k Vues
Learn about the anatomical considerations and surgical techniques involved in restoring acquired defects of the hard palate in dentate patients. Explore classifications of maxillectomy, lining the defect with skin grafts, obturator prosthesis design considerations, and principles of support, retention, and stability.

E N D
Restoration of acquired defects of hard palate in dentate patients Part II Hemant Jivnani JR II
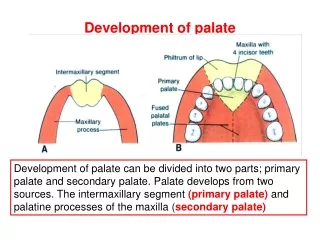
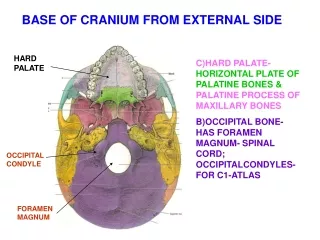
Brief anatomy of the maxilla, the palate and the maxillary sinus
Maxillectomy • Several different subtypes of maxillectomy have been described and due to the use of many terms like radical, total, subtotal, limited, partial, medial, extended maxillectomies; there has been a confusion regarding the nomenclature. • Maxillectomies can be classified according to spiro et al. based on the number of walls as • Limited: one wall • Subtotal: at least two walls including the palate • Total : resection of the entire maxilla
Line the reflected cheek flap with a split-thickness skin graft
If the wound is allowed to epithelialize spontaneously, it results in formation of poorly keratinized epithelium or respiratory epithelium which can not be utilized to obtain support, retention or stability for the obturator. While lining the defect with skin graft provides a highly keratinized surface that can be used to obtain support and retention for the obturator prosthesis on the defect side.
To remove the entire soft palate if less than one-third of the posterior aspect of the soft palate is to remain post surgically. (unless the patient is edentulous)
Imbibing the residual fibers of the levator veli palatini muscle within the lateral wall of the pharynx can enhance the residual velopharyngeal mechanism and an obturator can aid it to achieve velopharyngeal closure during swallowing along with a decreased hypernasality in speech.
Bony cut Palatal incision Save some of the palatal mucosa normally included in the resection and use it to cover cut medial bone margin of the palatal bones.
The need for support, retention and stability in designating any prosthesis should be understood if the objective of prosthodontic care are to be attained. For the patient with an acquired maxillary defect it is often necessary to modify, and sometimes violate, some of the basic principles of prosthesis design because of the basic nature of the defect. The remaining structure are most often unilateral, thus encouraging movement of the prosthesis with associated stress directed to these remaining structures.
The frequent location of unilateral remaining structures suggests that the obturator portion of the prosthesis, in addition to the residual structures, must contribute significantly to the support, retention, and stability of the prosthesis to satisfy the basic prosthodontic objectives.
SUPPORT Support is the resistance to movement of a prosthesis toward the tissue. The support available from the residual maxilla and from within the defect both must be considered. Residual maxilla support In the residual maxilla the primary areas available for support are the residual teeth, the alveolar ridge and the residual hard palate.
Residual teeth Carious involvement of the remaining teeth should be treated and their periodontal status made optimal. Support is also provided by the placement of occlusal rests, cingulum rest and incisal rest. Maximum effort should be directed toward saving as many teeth as possible without compromising the tumor resection protocol.
Within-the-defect support Positive support within the defect to prevent rotation of the prosthesis into it must be considered. This support can be achieved by contact of the prosthesis with any anatomic structures that provides a firm base. In most acquired maxillary defects the floor of the orbit, the bony structures of the pterygoid plate, and the anterior surface of the temporal bone near the infratemporal fossa are considered for positive support.
Floor of the Orbit Use of the floor of the orbit for support should be minimal. It cannot be used for support, if orbital floor has been removed then the orbital contents will move with the movement of the prosthesis. Drawbacks: If prosthesis is extended up to the orbital floor it would make insertion through the oral opening difficult, unless a two piece sectional prosthesis is used. Additional weight Problems of fabrication Alteration in speech quality due to too much obturation of the resonating chamber.
Pterygoid Plate or Temporal Bone Positive contact of the prosthesis with this bony structure can be relatively extensive and adequate to tripod the support for an obturator prosthesis.
The Nasal Septum It is a poor support for extensive prosthesis because, It is partly cartilage Has little bearing area Is covered with nasal epithelium.
RETENTION Retention is the resistance to vertical displacement of the prosthesis. • Retention is provided by • Within the residual maxilla • Within the defect • Residual Maxilla Retention-is provided by teeth in a dentate patient. • If the defect is small and remaining teeth are stable, intra coronal retainer can be used. ii) If the defect is large and all teeth are weak, extra coronal retainers should be used.
i) If the defect is small and remaining teeth are stable, intra coronal retainer can be used. ii) If the defect is large and some or all teeth are weak, extra coronal retainers should be used.
Within the defect retention Retention of an obturator prosthesis cannot be totally and adequately provided by the residual maxillary structures in either the edentulous or the dentulous patient unless the defect in exceptionally small. Large defects that approach the extent of the hemimaxillectomy must contribute intrinsically to the retention of the obturator prosthesis if the objectives of prosthesis design and prosthodontic care are to be achieved.
If the obturator extension itself could minimize the vertical displacement of the prosthesis, less stress would be generated to the residual maxillary structures. The following structures should be considered for retention within the defect. • Residual soft palate • Residual hard palate • Anterior nasal aperture • Lateral scar band • Height of lateral wall
Residual soft palate • Provides posterior palatal seal and minimizes passage of food and liquid above the prosthesis. • Extension of the obturator prosthesis onto the nasopharyngeal side of the soft palate provides retention.
B) Residual Hard Palate • Under cuts along the line of palatal resection into, nasal or para nasal cavity or medial wall of defect can increase retention. • Obturator extension into the undercut is best provided by a soft denture base material. • The extension shouldn’t contact the nasal septum or the turbinates
C) Lateral Scar Band For adequate surgical closure, most maxillary resections are lined with split – thickness skin graft along the anterior lateral and postero – lateral walls of defects. This results in the formation of scar band which is more prominent in laterally and postero – laterally as compared to scar band anterior to premolar region. These act as good undercuts for retention.
D) Height of lateral wall Engaging lateral wall of defect provides indirect retention. Longer radius undergoes less vertical displacement than the shorter radius.
STABILITY Stability is the resistance to prosthesis displacement by functional forces. Because function tends to move an obturator prosthesis, the principles of obturator design that minimize rotation around the horizontal plane and minimize movement within the horizontal plane itself must be considered. Rotation of the prosthesis around the horizontal plane is that rotation seen around the fulcrum line. Many aspects of obturator design are important to both retention and stability.
Movement of the prosthesis within the horizontal plane can be anteroposterior, mediolateral, rotational, or a combination of any or all of these directions. As with retention and support specific areas of the residual maxilla, as well as the defect itself, must be considered in minimizing the extent of these potential movements. Residual maxilla If natural teeth remain, the bracing components of the prosthesis framework can be used to minimize movement in all three directions.
It is advantageous to provide maximal bracing and to extend this bracing interproximally when possible to minimize rotational as well as anteroposterior movement of the prosthesis.
Within the defect stability The defect itself must be considered to enhance the stability of an obturator prosthesis. Maximal extension of the prosthesis in all lateral directions must be provided. Special emphasis must be placed on maximal contact with the medial line of resection, the anterior and lateral walls of the defect, the pterygoid plates, and the residual soft palate. Contact of the obturator portion of the prosthesis with these structures minimizes anteroposterior, mediolateral and rotational movement of the prosthesis.
Occlusion Occlusion is a very important aspect for stability of the prosthesis. an unstable prosthesis is the result if the occlusal relationship fails to maintain intimate contact of the prosthesis with the supporting and the retentive structures. To minimize the movement of the prosthesis, maximum distribution of occlusal forces is essential. Mastication over the defect should be avoided.
Purpose of the prosthetic dentition on defect side: Esthetic display Lip support Prevent opposing dentition from super-erupting Occlusal scheme Centric only contact on the defect side is preferred. Lateral interferences should be removed.
General considerations concerning the bulb design • A bulb is not necessary • Small to average size defect • Surgical or immediate temporary prosthesis • Need of hollow • To aid in speech resonance • Light weight
It should not be high as to cause the eye to move during mastication It should be closed superiorly always It should not be large as to interfere with insertion if the mouth opening is restricted.
General requirements of the framework design for obturator prosthesis, similar to that of a conventional removable partial denture A rigid major connector. Guide planes and other components that facilitate stability and bracing Rests that place supporting forces along the long axis of the abutment tooth
Direct retainers that are passive at rest and provide adequate resistance to dislodgment without overloading the abutment teeth Control of the occlusal plane that opposes the defect, especially when it involves natural teeth.
Unique considerations of the obturator framework The location and size of the defect, especially as it relates to the remaining teeth. The importance of the abutment tooth adjacent to the defect, which is critical to the support and retention of the obturator prosthesis. The usefulness of the lateral scar band, which flexes to allow insertion of the prosthesis but tends to resist its displacement and The use of the surveyor to examine the defect for the purpose of locating and preserving useful undercuts or eliminating undesirable undercuts.
Class 1- curved arch from Tripodal design is recommended if the anterior teeth are to be used for support or retention Linear design is recommended if the anterior teeth are not to be used for support or retention. Support Support for the prosthesis can be derived from: the remaining teeth, the residual palate, and the structures in the defect that may be contacted.
Rests: on most anterior and the mesiocclusal surface of the most distal abutment tooth when alignment and occlusion will permit. The mesiocclusal posterior rest, most often located between adjacent posterior teeth, is accompanied by a rest on the distoocclusal surface of the more anterior adjacent tooth. Since the prosthesis will first contact the undercuts and the other support areas, during insertion and the teeth will be engaged later, the prosthesis needs a compound path of insertion.
Guide planes will assist in the precise placement of the prosthesis once the teeth have been contacted. They will also ensure more predictable retention and add a greater degree of stability to the prosthesis. Guide planes on the anterior abutment should be kept to a minimum vertical height (1 to 2 mm) to limit torque on the abutment teeth and should be physiologically adjusted. This is important since movement can be expected during function because of the extensive lever arm provided by the defect and the dual nature of the support system.