Download
1 / 31
310 likes | 511 Vues
GROUP A STREP INFECTIONS IN CHILDREN 2/23/10. Benign to Moderate Upper resp tract carriers Impetigo Tonsillopharyngitis Scarlet Fever Streptococcal childhood fever. Serious and Severe Rheumatic Fever Acute Nephritis Toxic Shock Syndrome Necrotizing Fasciitis Sepsis/Focal infection.

E N D
Benign to Moderate Upper resp tract carriers Impetigo Tonsillopharyngitis Scarlet Fever Streptococcal childhood fever Serious and Severe Rheumatic Fever Acute Nephritis Toxic Shock Syndrome Necrotizing Fasciitis Sepsis/Focal infection GAS Spectrum of Illness
PHARYNGITIS in Children • 7.3 Million outpatient visits/yr • 96 antibiotic scrips written per 1000 US children < 15 yr age • Viruses cause 70-85% of acute pharyngitis and are benign/self-limited • Group A Streptococcus (Streptococcuspyogenes, GAS) causes 15-30%
VIRAL CAUSES of PHARYNGITIS • Rhinovirus, coronavirus (common cold) • Parainfluenza (common cold, croup) • Influenza A and B (common cold, flu) • Adenovirus (pharyngoconjunctival fever) • Herpes simplex types 1 and 2 (gingivostomatitis) • Coxsackievirus A, other enteroviruses (HFM disease, herpangina) • EBV, CMV (mono syndromes) • HIV (primary infection)
BACTERIAL CAUSES of PHARYNGITIS • Group A Streptococcus (scarlet fever) • Groups C and G • Neisseria gonorrhoeae • Corynebacterium diphtheriae (diphtheria) • Arcanobacterium haemolyticum (scarletiniform rash) • Yersinia enterocolitica (enterocolitis) • Yersinia pestis (plague) • Francisella tularensis (tularemia, oropharyngeal) • Mixed anaerobes (Vincent’s angina)
OTHER CAUSES of PHARYNGITIS • Mycoplasma pneumoniae • Chlamydophila psittaci • Chlamydophila pneumoniae • ? Others
Suggesting GAS Sudden onset sore throat and fever Scarletiniform rash 10% Headache N, V, abd pain Exudate on tonsils Palatine petechiae Tender/enlarged nodes Age 5-15 years Winter, early spring History of exposure Excoriated nares < 3 Suggesting viral etiology Cough, coryza Conjunctivitis Diarrhea Characteristic rash Characteristic enanthem From Bisno et al. Clin Infect Dis 2002;35:113-25 Clinical/Epidemiologic findings
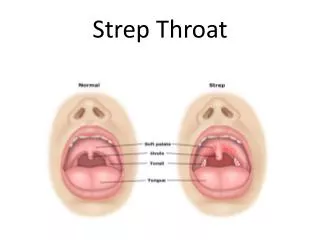
Diagnosis of GAS Pharyngitis • Clinical diagnosis is easy in the 5-15 yr old child in winter,early spring with classic sudden onset sore throat, fever, HA and beefy red uvula, pus on tonsils, tender, enlarged AC nodes, and a scarletiniform rash • BUT, none is specific for GAS and rarely do you see all of these together
Any or none could be GAS • Symptoms and signs overlap broadly • Bacteriologic confirmation required • WHO should we test? -- ALL suspects • HOW should we test? -- RST and Culture
Diagnosis of GAS Pharyngitis THROAT CULTURE IS THE GOLD STD • Sensitivity of about 95-99% with blood agar and aerobic incubation at 35-370 for 18-24 hr • Both tonsils and posterior wall should be sampled
Diagnosis of GAS Rapid Antigen Detection Testing • Specificity 95%-99% • Sensitivity 80-90% (vs. BAP culture) • False negatives are not merely carriers • False positives may be due to S. milleri • Negative tests allows no AB RX • NEED BACKUP CULTURE
Case 1: March, 6 yr old child, 2 day hx of sore throat and headache, no cough or coryza. On exam, he is febrile, his pharynx is erythematous with pus on this tonsils, and he has tender cervical adenopathy.How to approach?
ST, HA, FEVER in MARCHOPTIONS 1. No tests -- Rx on clinical criteria 2. No tests -- no Rx 3. RST -- if pos, Rx -- if neg, no Rx, no TC. -- if neg, do TC and Rx awaiting TC, stop Rx if TC neg -- if neg, do TC and Rx only if TC pos 4. TC -- RX awaiting TC, stop Rx if TC neg. -- Rx only if TC pos. 5. RST and/or TC, continue Rx despite neg result
ST, HA, FEVER in MARCH OPTIONS 1. No tests -- Rx on clinical criteria 2. No tests -- no Rx 3. RST -- if pos, Rx -- if neg, no Rx, no TC. -- if neg, do TC and Rx awaiting TC, stop Rx if TC neg -- if neg, do TC and Rx only if TC pos 4. TC -- RX awaiting TC, stop Rx if TC neg. -- Rx only if TC pos 5. RST and/or TC, continue Rx despite neg result
Case 2: July, 6 yr old child, 2 day hx sore throat and coryza but no cough. On exam, he is afebrile, his pharynx is erythematous but there is no pus on his tonsils and he has no adenopathy.
ST, CORYZA, NO FEVER in JULY OPTIONS 1. No tests -- Rx on clinical criteria 2. No tests -- no Rx 3. RST -- if pos, Rx -- if neg, no Rx, no TC. -- if neg, do TC and Rx awaiting TC, stop Rx if TC neg -- if neg, do TC and Rx only if TC pos 4. TC -- RX awaiting TC, stop Rx if TC neg. -- Rx only if TC pos. 5. RST and/or TC, continue Rx despite neg result
ST, CORYZA, NO FEVER in JULY OPTIONS 1. No tests -- Rx on clinical criteria 2. No tests -- no Rx 3. RST -- if pos, Rx -- if neg, no Rx, no TC. -- if neg, do TC and Rx awaiting TC, stop Rx if TC neg -- if neg, do TC and Rx only if TC pos 4. TC -- RX awaiting TC, stop Rx if TC neg. -- Rx only if TC pos 5. RST and/or TC, continue Rx despite neg result
Clinical Pearls: Strep Pharyngitis • 80 % NPV if cough, rhinorrhea, hoarseness; no fever, pus, or nodes • Natural hx of untreated illness is resolution in 3-5 days (self-limited) • Not a benign illness in children (suppurative and non-suppurative sequelae are possible) a) AGN b) ARF
YOUNG CHILDREN WITH STREP • Streptococcal childhood fever, streptococcosis, excoriated nasopharyngitis • Intertrigo
Treatment of GAS Pharyngitis Reasons for treating • Shortens clinical illness by about 24 hr • Prevention of suppurative complications like peritonsillar abscess, adenitis, NF) • Prevention of non-suppurative complications like ARF (NOT AGN or PANDAS) • Prevention of transmission to contacts
Treatment of GAS Pharyngitis is Primary Prevention of ARF • Rheumatogenic strains and genetic predisposition for ARF to follow GAS • Only Bicillin has been shown to prevent ARF (in 1950s) • Now we equate bacteriologic eradication with likely prevention of ARF in trials • Up to 9 days to treat
All GAS susceptible to penicillins and cephalosporins usually susceptible to clindamycin Penicillin is still Rx of choice Macrolide resistence is rising in US LIMITED VALUE: sulfa, tetracyclines, chloramphenicol, aminoglycosides Antibiotic Treatment
Antibiotic Treatment for Strep Pharyngitis/Prevention of ARF • Oral Penicillin V 250 bid or tid for 10 days in children and 500 bid or tid for adolescents or adults is standard • QD or 5-7 days is not acceptable • Amoxicillin bid or tid often used for taste • Bicillin lasts (bactericidal levels) 21-28 d • Once-daily Amoxicillin is effective, not FDA approved, but accepted/endorsed (50 mg/kg once daily; maximum 1 g)
Cephalosporin Antibiotic Treatmentfor Strep Pharyngitis • Indicated if allergic to Pen and rxn not IG E –mediated (new) • May be better for eradication of GAS • Cost, broader coverage limit use • Ceftriaxone may have a role if vomiting
Other Antibiotics for StrepPharyngitis Approved by FDA • Azithromycin x 5 days 10-12 mg/kg/day and NOT as for OM • Cefpodoxime 10/mg/kg/day bid 5 days • Cefdinir 7 mg/kg/day bid 5 days • Augmentin
Carrier state eradication • Clindamycin 20/mg/day div tid 10 days (max 1.8 gm/day) • Penicillin plus rifampin last 4 days of Rx
Tonsillectomy indications • 6 GAS infections in 1 year • 3-4 GAS infections in each of 2 years
REFERENCES • Gerber et al. Prevention of Rheumatic Fever and Diagnosis and Treatment of Acute Streptococcal Pharyngitis: A Scientific Statement From the American Heart Association…Circulation. 2009;119:1541-1551. (Endorsed by the AAP) • Bisno et al. Practice Guidelines for the Diagnosis and Management of Group A Streptococcal Pharyngitis. Clin Infect Dis. 2002;35:113-125. (in revision) • Red Book 2009 • Kaplan et al. Anti-streptolysin O and Anti-deoxyribonuclease B Titers: Normal Values for Children Ages 2-12 in the United States. Pediatrics. 1998;101: 86-88.