Download

1 / 6
90 likes | 393 Vues
TRITON-TIMI 38. Trial to assess improvement in therapeutic outcomes by optimizing platelet inhibition with prasugrel-thrombolysis in myocardial infraction 38 trial. Wiviott S.D et al. N Engl J Med 2007 ; 357 : 2001-15. Méthodologie. Objectif

E N D
TRITON-TIMI 38 Trial to assess improvement in therapeutic outcomes by optimizing platelet inhibition with prasugrel-thrombolysis in myocardial infraction 38 trial Wiviott S.D et al. N Engl J Med 2007 ; 357 : 2001-15.
Méthodologie Objectif Comparaison de 2 AAP prasugrel-clopidogrel (thiénopyridines, inhibiteurs ADP) associés à l’aspirine pour ATL programmée dans les suites du SCA Etude Étude randomisée, en double insu, multicentrique Critèresd’inclusion ATL coronaire programmée pour SCA ST+/- Aspirine systématique TRITON-TIMI 38 AAP = antiagrégant plaquettaire ATL : angioplastie transluminale SCA = syndrome coronaire aigu Wiviott S.D et al. N Engl J Med 2007 ; 357 : 2001-15.
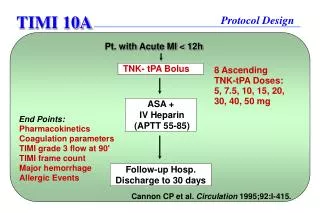
Schéma de l’étude Clopidogrel : DC 300 mgpuis 75 mg/jn = 6795 ATL coronaire programmée pour SCA ST+/- Aspirine systématique (n=13608) Critère de jugement principal Mortalité CV, IDM, AVC TRITON-TIMI 38 R Prasugrel : DC 60 mgpuis 10 mg/jn = 6813 ATL=angioplastie transluminale SCA : syndrome coronaire aigu Wiviott S.D et al. N Engl J Med 2007 ; 357 : 2001-15.
Résultats • Efficacité et tolérance Clopidogrel 12,1 % Prasugrel 9,9 % TRITON-TIMI 38 2,4 % 2,4 % 1,8 % 1,1 % p < 0,001 p < 0,001 p = 0,03 Hémorragies graves Thrombose endoprothèse Critère I : mortalité CV, IDM, AVC IDM = infarctus du myocarde AVC= accident vasculaire cérébral Wiviott S.D et al. N Engl J Med 2007 ; 357 : 2001-15.
Résultats • Analyse de l’effet d’une coprescription d’IPP* (à la discrétion du médecin) au prasugrel ou clopidogrel sur le risque cardiovasculaire (n = 4529, 33% population étude) 14 Sans IPP Clopidogrel 12 IPP IPP TRITON-TIMI 38 10 Prasugrel Sans IPP 8 Décès CV, IDM, AVC (%) 6 4 Clopidogrel IPP vs sans IPP : RR ajusté 0,96 (IC95 : 0,82-1,12) 2 Prasugrel IPP vs sans IPP : RR ajusté 0,99 (IC95 : 0,83-1,17) 0 0 100 200 300 400 Jours * Pentoprazole 40%, oméprazole 37%, ésoméprazole 14%, lansoprazole 9,7%, rabéprazole 1,5% Wiviott S.D et al. N Engl J Med 2007 ; 357 : 2001-15.
Conclusion • Prasugrel : efficacité significativement supérieure au clopidogrel pour diminuer mortalité CV, IDM, AVC après ATL programmée pour SCA au prix d’un surcroît significatif d’hémorragies graves • Aucun effet indésirable CV de l’association IPP-AAP type Prasugrel ou Clopidogrel MAIS prescription IPP non randomisée TRITON-TIMI 38 Wiviott S.D et al. N Engl J Med 2007 ; 357 : 2001-15.