Download
1 / 56
560 likes | 602 Vues
Explore the intersection of HIV/AIDS and TB with a focus on prevention and treatment challenges, in light of the era of antiretroviral treatment scale-up. Learn about the overlapping epidemiology, resources, and the urgent need for action. Health development evolution and the shift towards recognizing health as a human right and vital investment are discussed, along with the international efforts to combat these deadly diseases. Discover the impact of the HIV epidemic worldwide and the urgent need for coordinated responses. Join the conversation on health, human rights, and sustainable development.

E N D
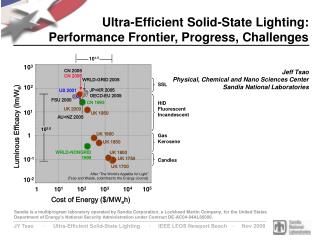
HIV/TB 2005 • HIV/AIDS, TB and malaria high on the agenda of human development • New and important resources available • Overlapping epidemiology • Challenges of preventing and treating TB in HIV/TB co-infected patients in the era of antiretroviral (ART) treatment scale up
26-27 SEPTEMBER 2005 • « Drug resistance combined with a deadly double infection of TB and HIV is posing a serious threat in Cambodia, Vietnam, China and thePhilippines », said the WHO … (Noumea, 27 September) • « The WHO last month declared a tuberculosis emergency for Africa, where the rate of infection has quadrupled in many countries since 1990. The epidemic kills more than 500,000 Africans each year » …(Cape Town, 26 September)
HEALTH AND HUMAN DEVELOPMENT • In the sixties and early seventies : emphasis on the fight against large endemics (malaria, yellow fever, leprosy) and on building and supporting hospitals in capital cities. • In the eighties and early nineties : the rapid demographic growth, economic crisis and persistence of the major infectious diseases further weaken the sanitary situation in developing countries. • Developing countries cannot afford the necessary and increasing costs of health; the health sector is left aside in « structural adjustement » policies.
HEALTH AND HUMAN DEVELOPMENT • Mid-nineties : health is accepted as a human right and increasingly considered as a « Global Public Good ». • Mid-nineties : health is increasingly seen as integrated with other developmental issues such as clean water, human rights, governance; decade of United Nations Conferences on Human rigths (1990 Children Summit, 1994 Cairo Summit on Population, 1995 Beijing Conference on Women). • The debate around the relationship between inequality and poverty further leads to the realization that economic development cannot occur without access to human rights including access to health.
HEALTH AND DEVELOPMENT • End of the nineties, early two thousands : The AIDS crisis leads to realize that health should not be considered anymore as a consequence of development but as a factor for development, particularly through preservation of « human capital ». • The health sector originally considered as a non-profitable source of expenditure becomes increasingly understood as a necessary investment.
Health on the international agenda • 2000 : Health is brought to the agenda of the G8 in Okinawa. • 2000 : Three of the Millenium Development Goals (MDG Summit) relate to health : reduce child mortality, improve maternal health, combat HIV/AIDS, malaria and other diseases • 2001 : UNGASS • 2002 : Global Fund to fight AIDS, malaria and TB • 2005 : declaration on Universal access to treatment of HIV/AIDS by 2010 (Gleneagles G8 and MDG summit in New York)
HIV/AIDS 1996 : 300 millions $ 2001 : 2,1 billions $ 2004 : 6,1 billions $ 2005 : 8 billions $ TB for 22 HBC countries* 2002 : 850 millions $ 2003 : 950 millions $ 2004 : 1,1 billion $ 2005 : 1,3 billion $ * representing 80% of patients Global resources for HIV/AIDS and TB
TB (Rounds 1-5) 95 grants 72 countries 1.6 Billion $ 66% global external resources HIV/AIDS (Rounds1-5) 135 grants 124 countries 5,19 Billions $ 25-30% global external resources Global Fund support
HIV INFECTION WORLDWIDE 2005 • Number of people living with HIV : 39.4 M (35.9-44.3) • New HIV infections : 5 million/ year ; 570 /hour ; 10/ minute Half among young adults aged 15-24 Half in women 90% in low resource-settings
HIV INFLICTS DEATH SLOWLY • For three decades, the epidemic has created waves of infection, followed years later by waves of acute infection, and years after by waves of death. Intervals between these waves have lasted up to 10-15 years and the waves themselves have been staggered with the progression of infection varying from person to person. • Successive high amplitude waves have swept sub-Saharan Africa for over 30-35 years and up to four human generations in the Great Lakes region. Botswana, Malawi and Western Africa are now in a third generation of low amplitude waves. • South Africa has yet to experience the full death tolls of their first wave of infection. On the other hand, low amplitude waves have gone almost unnoticed for ten years or more in India, Indonesia, China, and Russia. Illness, death and orphans are still ahead.
Impact d’une épidémie hors contrôle • Impact démographique • Impact économique • Impact sur le développement
OVERLAPPING EPIDEMIOLOGY OF HIV INFECTION AND TUBERCULOSIS TB is the first cause of morbidity and mortality in HIV-infected adults in the developing world. • In the last four years, > 11 % of all new TB cases in adults each year, occurred in persons infected with HIV. • 12 % of the 2 million deaths from TB were attributable to HIV. • >10 % of all AIDS-related deaths were caused by TB. In some sub-Saharan countries, TB causes over one third of AIDS-related deaths .
TUBERCULOSIS AND ANTIRETROVIRAL THERAPY (1) • ART associated with > 80 % decrease in incidence of HIV-associated TB in TB-endemic areas • Protective effect of ART greatest in symptomatic patients and those with advanced disease. • Concurrent use of ART with TB- treatment associated with reduced mortality.
CLAIMS THAT OPPOSE TREATMENT • Prevention should be a priority over treatment • Antiretroviral treatment is not affordable • Antiretroviral treatment is not cost-effective • Effectiveness, tolerance and adherence unknown • Lack of infrastructures • Risk of dissemination of resistant viral strains • Concern over equity
ART-LINC vs. ART-CC: Cumulative mortality at month 12of antiretroviral therapy (Weibull) ART-LINC (167 deaths / 3177 PYFU) ART-CC (155 deaths / 11758 PYFU) 12 12 10 10 8 8 Probability of death (%) 5.8 % Probability of death (%) 6 6 4 4 1.6 % 2 2 0 0 0 3 6 9 12 0 3 6 9 12 Months from starting HAART Months from starting HAART
TUBERCULOSIS AND ANTIRETROVIRAL THERAPY IN SUB SAHARAN AFRICA • Incidence is decreased in adult patients receiving ART as compared with those not receiving it. • Incidence of active TB remains however higher in ART-treated patients than in HIV-negative individuals 1. • TB remains the most common cause of intermediate-term severe morbidity in adults receiving ART 2. 1Badri, Lancet 2002; 2Seyler C, Antivir Ther, 2003
TUBERCULOSIS AND ANTIRETROVIRAL THERAPY (2) • Tuberculosis incidence and recurrence rates remain high in HIV-infected patients receiving ART. • Risk of active TB in ART-treated patients is significantly higher in patients with a previous history of TB (11.3/100 persons-years) than in those without prior tuberculosis (3.0/100 persons-years) 1. 1Seyler, Am J Resp Crit Care Med, 2005
ANTIRETROVIRAL THERAPY ALONE WILL NOT SOLVE AFRICA’S TB EPIDEMIC 1 • Current guidelines initiate ART late in HIV disease when much of the HIV-associated TB burden has already been experienced. • ART will allow more persons to be alive with systemic immunosuppression and high vulnerability to primary and recurrent TB. 1De Cock KM, Am J Resp Crit Care Med, 2005
CHALLENGES OF CONCOMITANT ART AND TB THERAPY (1) • TB treatment is to be started immediately following TB diagnosis. • Decision on when to initiate ART depends on balancing the risk of « immune reconstitution syndrome1 »/drug-drug interactions, with risk of HIV disease progression. • Prospective randomized studies on timing of ART are ongoing. 1 Enhanced anti-tuberculosis inflammatory responses in infected tissues resulting from restoration of pathogen-specific immunity.
HRZE (2 months) RH (4 months) ARV Early R End of anti-TB Anti-TB Late ARV Day 1 Day 14M2M6M12
CHALLENGES OF CONCOMITANT HAART AND TB THERAPY (2) • Drug toxicity is a major cause of interrupting/discontinuing ART and/or TB therapy during concomitant treatment in co-infected patients. • Rifampicin-based regimens are associate with betterc responses to treatment in HIV-TB co-infected patients 1. Plasma concentration of non nucleoside reverse transcriptase inhibitors (NNRTIs) and protease inhibitors (PIs) is decreased during concomitant treatment with rifampicin. 1 Use of RFP to be based on 2004 revised WHO guidelines;
CHALLENGES OF CONCOMITANT HAART AND TB THERAPY (3) • DOT therapy vs self-administered therapy for the treatment of TB • DOT to deliver ART • Rigorous assessment of ART combined with TB DOT still needed
TUBERCULOSIS AND ANTIRETROVRAL THERAPY IN DEVELOPING COUNTRIES • Neither better performing tuberculosis programs alone, nor implementing ART programs that would ignore the HIV-uninfected sources of TB transmission, will control tuberculosis in developing countries where TB is driven by HIV infection. • There is an urgent need in these countries, for implementation of combined and coordinated diagnostic, preventive and therapeutic interventions for HIV and TB.
IMPORTANT STEPS TO IMPROVE CARE OF HIV-TB CO-INFECTED PATIENTS IN THE DEVELOPING WORLD • Implement universal HIV testing of patients diagnosed with TB (HIV prevalence > 5 %) • Exclude active TB in patients diagnosed with HIV infection • Provide co-trimoxazole therapy to TB patients with HIV infection • Offer access to ART and long term HIV care to TB patients with HIV infection
IMPORTANT STEPS TO IMPROVE CARE OF HIV-TB CO-INFECTED PATIENTS : THE RESEARCH AGENDA1 • TB prophylaxis in HIV-infected persons • Cotrimoxazole prophylaxis • Time of initiating ART • Intensified case-finding focus and improving TB/HIV collaborative activities • New tools and diagnostic algorithms to improve the diagnosis of smear-negative TB in adults and children • Shorter duration TB treatment regimens • New and affordable drugs for TB and MDR TB 1 WHO, 2005
IMPROVING TB TREATMENT OPTIONS FOR HIV-TB CO-INFECTED PATIENTS • Globally, 40 % of diagnosed TB patients fail to complete therapy. • Poor adherence associated with long (6-8 months) regimens. Shorter duration regimens would improve treatment completion rates. • Regimens that can easily be given with ART urgently needed.
OCTOBER 2005/ FIRST QUARTER OF 2006 • TB/HIV research priorities in resource-limited settings • Updated Stop-TB strategy 1 • Global plan of action 2006-2015 for the Stop-TB partnership 1(1) quality DOTS expansion and enhancement; (2) TB-HIV and MDR TB; (3) health systems strengthening ; (4) engage all care providers; (5) patients and community; (6) research
HIV INFLICTS DEATH SLOWLY • For three decades, the epidemic has created waves of infection, followed years later by waves of acute infection, and years after by waves of death. Intervals between these waves have lasted up to 10-15 years and the waves themselves have been staggered with the progression of infection varying from person to person. • Successive high amplitude waves have swept sub-Saharan Africa for over 30-35 years and up to four human generations in the Great Lakes region. Botswana, Malawi and Western Africa are now in a third generation of low amplitude waves. • South Africa has yet to experience the full death tolls of their first wave of infection. On the other hand, low amplitude waves have gone almost unnoticed for ten years or more in India, Indonesia, China, and Russia. Illness, death and orphans are still ahead.
PULMONARY COMPLICATIONS OF HIV INFECTION IN ADULT PATIENTS IN SUB-SAHARAN AFRICA • TB is the first on the list of differential diagnoses of patients who present to the health care system with chronic cough and other pulmonary symptoms. • As HIV disease and immune deficiency progress, the clinical and radiographic manifestations of TB become increasingly atypical.
Global Task Teamon improving AIDS Coordination among Multilateral Institutions and International Donors • Gathered donor and developing country governments, civil society, UN agencies and other international institutions • Developed recommendations within 80 days on improving the institutional architecture of the response to AIDS/HIV • In line with the « three ones » principles and with the Paris Declaration on Aid effectiveness • Recommendations were to inform the replenishment process of the Global Fund.
GTT recommendations 1 • Countries develop annual priority AIDS action plans that drive implementation and provide a base for the alignment of multilateral/international partners’ support • WB/UNDP/UNAIDS provide support on the integration of AIDS into PRSPs • Multilateral/international partners commit to working with national AIDS coordinating authorities to align their support to national strategies (Joint annual reviews) • Shift from project to programme financing (GF and WB for joint programmatic and financial reporting)
GTT recommendations 2 • The UN resident coordinator will establish a joint UN team on AIDS to develop a unified UN country programme • The multilateral system with GF establish a joint UN system Problem-solving team to address implementation bottlenecks at country level • UNAIDS cosponsors and the Global Fund establish a clearer division of labour based on their comparative advantages and complementarities
Perspectives to maximise the synergies between HIV/AIDS and TB 1 • Keep two separates programmes at national level but opportunities to create synergies between the two systems (parallelism of the two diseases : long term disease / biological specificities (need laboratories) / multi therapy / resistances • TB is a good opportunity to test and reach HIV/AIDS infected persons (stigmatisation?) and other way round
Perspectives to maximise the synergies between HIV/AIDS and TB 2 • Would The « Global Drug Facility for TB » be a good example for HIV/AIDS? • How would GTT recommendations and/or 3/1 be adapted to TB programme (joint MEE, joint Technical Assistance training..) • What about the creation of a « Stop VIH/AIDS partnership »?
Perspectives to maximise the synergies between HIV/AIDS and TB 3 • Ensure to integrate « systematically? » a TB profil within each CCM • Elaborate, on the model of the Green light committee, an observatoire on resistance • Analyse why Global fund Tb grants/best performance?
PROPHYLAXIS OF HIV-RELATED TB • INH prophylaxis reduces TB incidence but not mortality. • Greatest effect among TST+ individuals. • Rifamycin-based regimens as effective as isoniazide prophylaxis. • Durability limited in high incidence settings • Prophylaxis still not widely used despite low cost.
Observance mensuelle moyenne en fonction de la durée de traitement chez 159 patients suivis de novembre 1999 à octobre 2003.
Distribution des motifs d’interruption prolongée de traitement (>6 jours) en fonction de l’année de suivi (N=159)
Study design - early = 2 weeks after the onset of anti-TB - late = 8 weeks after the onset of anti-TB - anti-TB treatment : according to the Cambodian National TB Program and the most recent state of the art (Lancet 2004) . initial phase = 2 months of rifampicin-isoniazid-pyrazinamide-ethambutol (HRZE) . continuation phase = 4 months of rifampicin-isoniazid (RH)
1996 – 2000 Improved understanding of pathogenesis Availability of quantitative assays of HIV RNA, cell-associated DNA, and assays for viral resistance More potent antiretroviral drugs Immune reconstitution with HAART
clinical latency progression seroconversion virus CD4 NATURAL HISTORY OF HIV DISEASE AIDS months Years
PROGRESSIVE LOSS OF TH FUNCTION IN HIV DISEASE CD4 cells/mm3 800 600 300 200 100 IL-2 production + +/- - - - Recall antigens + +/- - - - Allogeneic stimuli + + +/- - - Mitogens + + + +/- - B PWM + +/- - - -
HIV THERAPY ACHIEVEMENTS • Dramatic reduction in mortality • Dramatic reduction in morbitity and improvement in quality of life • Dramatic reduction in health care utilization • Insights into pathogenesis