Download
1 / 73
810 likes | 1.29k Vues
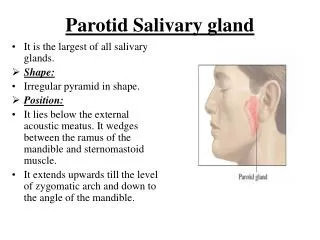
SUBMANDIBULAR SALIVARY GLAND. PROF PALANI MS FICS. P aired salivary glands that lie below the mandible on either side. larger superficial and a smaller deep lobe. D rained by a single submandibular duct (Wharton’s duct ).

E N D
SUBMANDIBULAR SALIVARY GLAND PROF PALANI MS FICS
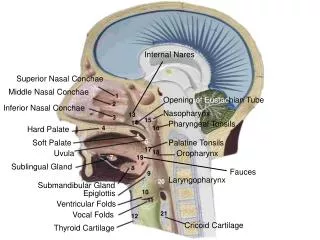
Paired salivary glands that lie below the mandible on either side. • larger superficial and a smaller deep lobe. • Drained by a single submandibularduct (Wharton’s duct). • It drains into the anterior floor of the mouth at the sublingual papilla.
Important anatomical relationships of thesubmandibular glands 3 NERVES—Marginal mandibular branch of facial nerve __hypoglossal nerve __lingual nerve 2 MUSCLES__mylohyoid __hyoglossus 1 ARTERY __facial artery.
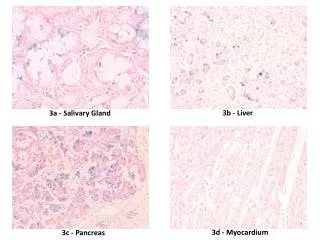
Ectopic/aberrant salivary gland tissue • most common ectopic salivary tissue is the Stafne bone cyst. • asymptomatic, clearly demarcated radiolucencyof the angle of the mandible. • Formed by invagination into the bone on the lingual aspect of the mandible of an ectopic lobe of the juxtaposed submandibulargland. • No treatment required.
INFLAMMATORY DISORDERS Acute, Chronic or Acute on Chronic. Acute submandibularsialadenitis: - Viral : The paramyxovirus (mumps). - bacterial : secondary to obstruction.
OBSTRUCTION AND TRAUMA • most common cause is stone formation. • Eighty per cent of all salivary stones occur in the submandibular glands because their secretions are highly viscous. • Eighty per cent of submandibularstones are radio-opaque and can be identified on plain radiography.
SYMPTOMS: • Acute painful swelling in the region of the submandibular gland, precipitated by eating. • Swelling occurs rapidly and often resolves spontaneously over 1–2 hours after the meal is completed—complete obstruction. • Minimal discomfort and swelling, not confined to mealtimes—partial obstruction.
SIGNS: • enlarged firm submandibular gland, tender on bimanual examination. • Pus may be visible, draining from the sublingual papilla.
TREATMENT: • DISTAL TO LINGUAL NERVE: -- INTRAORAL APPROACH. • PROXIMAL TO LINGUAL NERVE: -- gland excision, stone removal and duct ligation.
EXCISION • Incision and exposure of gland • Gland mobilisation. • Dissection of the deep lobe and identification of the lingual nerve. • Wound closure.
Incision and exposure of gland • Incision should be marked at least 3–4 cm below the lower border of the mandible to avoid damage to the marginal mandibular branch of the facial nerve. • Superficial veins, including the anterior facial vein, require ligation.
Gland mobilisation intracapsulardissection - inflammatory conditions extracapsulardissection -tumours.
Dissection of the deep lobe and identification of the lingualnerve • Important landmark in submandibular gland dissection is the posterior border of the mylohyoid muscle. • The gland is retracted inferiorly, invariably attached to the lingual nerve through parasympathetic secretor motor fibres. Lingual nerve preserved. • Duct ligated and gland excised.
Three cranial nerves are at risk during removal of the submandibular gland: 1 The marginal mandibular branch of the facial nerve. 2 The lingual nerve. 3 The hypoglossal nerve.
Complications of submandibular gland excision 1. Haematoma; 2. wound infection; 3. marginal mandibular nerve injury; 4. lingual nerve injury; 5. hypoglossal nerve injury; 6. transection of the nerve to the mylohyoid muscle producing submentalskin anaesthesia.
SUBMANDIBULAR GLAND TUMORS • Only 50%of submandibular gland tumours are benign, in contrast to 80–90% of parotid gland tumors. • In many circumstances, the swelling cannot, on clinical examination, be differentiated from submandibularlymphadenopathy. • Most salivary neoplasms, even malignant tumours, are often slow-growing, painless swellings.
ETIOLOGY • ENVIRONMENTAL : Radiation (ionising & UV radiation). EBV. Silica dust. Early menarche & nulliparity. Smoking (Warthin’s tumor). Diet rich in PUFA (protective) • GENETIC.
PLEOMORPHIC ADENOMA • most common benign tumor of both major & minor salivary glands. • Peak incidence 4th & 5th decade with slight female preponderance.
MICROSCOPY Epithelial & modified myoepithelial cellsintermingle with a stroma can be mucoid, myxoid, fibrous or chondroid. • Areas of oncocyticmetaplasiaare common & it can be misdiagnosed as oncocytoma. • Most characteristic appearance of stroma is the formation of mucoid or myxochondroid areas containing scattered epithelial cells with cartilaginous or osseous metaplasia.
Principal clinical problem is recurrence (3.4 % in 5 yrs – 6.8 % in 10 yrs) and malignant progression. • RISK FACTORS FOR RECURRENCE : Variable / Absent capsulation. Intracapsular invasion. Improper excision.
MUCOEPIDERMOIDCARCINOMA • MC malignant tumor of salivary gland.. • Low grade : predominance of mucous secreting cells with well differentiated epidermoid cells. • High grade : few or no mucous producing cells and poorly differentiated epidermoid cells.
ADENOID CYSTIC CARCINOMA • 15 % of salivary neoplasms. • 2nd most common malignant tumor of salivary glands. • MC malignant tumor in submandibular, sublingual & minor salivary glands. • Peak incidence 5th & 6ht decade. • MC site : oral cavity (50%) sinonasal tract (18%)
ACINIC CELLCARCINOMA • 5 – 11 % of malignant tumors of salivary glands. • Presents at a younger age. • Affects women > men. • Arises MC in parotid. • MICROSCOPY : cells with basophilic cytoplasm associated with lymphoid infiltrate. • Subtypes : solid, microcystic, papillary cystic & follicular
MALIGNANT MIXED TUMOR • Represents malignancy with both epithelial & mesenchymal elements. • 3 – 12 % of salivary gland tumors. • Carcinoma ex pleomorphic adenoma - arising from pre exsistingpleomorphic adenoma. Malignant & metastatic components are epithelial in origin. • De novo malignant mixed tumor (CARCINOSARCOMA) : with malignant features of both epithelial and mesenchymal components
Con………………. • malignant transformation occurs in 3 – 4 % of all benign mixed tumors. • Risk of malignant transformation of pleomorphic adenoma increases with duration of disease. ( 1.5% within 5 yrs - 9.5% within 15 yrs). • Features of malignancy in pleomorphic adenoma Necrosis, calcification, hemorrhage and excessive hyalinization.
Clinical features of malignant submandibulartumours 1. Rapid enlargement of the swelling. 2. Indurationand/or ulceration of the overlying skin. 3. Cervical node enlargement. 4. Ipsilateral weakness / numbness of tongue. 5. Fixity to mandible.
INVESTIGATIONS • FNAC [ sensitivity : 85 – 99 % specificity : 96 – 100% ] • Open surgical biopsy is contraindicated. • Trucut biopsy-inoperable tumor -lymphoma.