BACKGROUND
10 likes | 164 Vues
Macrolide Immunomodulation and Outcomes in Hospitalized Patients with Community-Acquired Pneumonia

BACKGROUND
E N D
Presentation Transcript
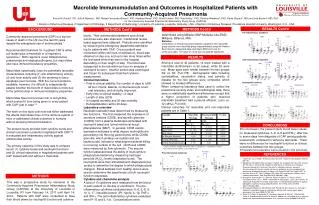
Macrolide Immunomodulation and Outcomes in Hospitalized Patients with Community-Acquired Pneumonia Forest W. Arnold1, DO, Julio A Ramirez1, MD, Rafael Fernandez-Botran2, PhD, Madhavi Rane3, PhD, Silvia Uriarte3, PhD, Rob Kelley1, PhD, Timothy Wiemken1, PhD, Paula Peyrani1, MD and Jose Bordon4, MD, PhD for the Community-Acquired Pneumonia Inflammatory Study Group (CAPISG) 1 Division of Infectious Diseases, 2 Department of Pathology, 3 Department of Nephrology, University of Louisville, Louisville, Kentucky, USA. 4 Section of Infectious Diseases, Providence Hospital University, Washington, D.C., USA RESULTS Cont’d METHODS Cont’d BACKGROUND METHODS Cont’d Pro-inflammatoryCytokines determined using Milliplex MAP Multiplex kits (EMD Millipore, Billerica, MA). Statistics Comparison of clinical outcomes between subjects in the macrolide group and the non-macrolide group was performed using the Fisher’s Exact test for categorical data, and Mann-Whitney U test for continuous data. A P value of <0.05 was considered significant. • levels. Their antimicrobial treatment and clinical outcomes were also observed. Institutional review board approval was obtained. Patients were identified by screening the emergency department admission log for patients with CAP. Once a patient was consented (within 48 hours of admission), blood was obtained on day one, and up to two more times within the first week while they were in the hospital depending on their length of stay. The blood was transported to the lab within an hour for analysis of neutrophil function. Another portion was centrifuged and frozen for subsequent batched cytokine measurement. • Clinical Outcomes • Time to clinical stability: the number of days to fulfill • all four criteria: afebrile, normal leukocyte count, • oral toleration, and clinically improved. • Early time to clinical stability: <3 days • Length of stay (LOS) • In-hospital mortality and 30-day mortality • Rehospitalization within 30 days. • Laboratory overview • Neutrophil activation was determined by measuring two functions. The first measured the expression of secretory vesicles (CD35), and specific granules (CD66b) from a plasma membrane stimulated with neutrophil basal and formyl-methionyl-leucyl-phenylalanine (fMLF). In general, CD35 vesicle expression indicates to what degree neutrophils are penetrating into the lung parenchyma, while CD66b granules, which undergo exocytosis and are bacteriocidal, indicate to what degree bacterial killing is occurring outside of the cell. CD35 and CD66b were measured by flow cytometry. The second function assessed was the ability of neutrophils to phagocytose bacteria by measuring hydrogen peroxide (H2O2) levels (respiratory burst). The neutrophils were then stimulated with Staphylococcus aureusto determine the degree to which phagocytosis changed. Blood samples from healthy donors were used to determine the basal levels of both neutrophil function responses. • Cytokine and chemokine analysis • A total of 10 cytokines were measured from the blood of each patient on the day of enrollment. The pro-inflammatory cytokines evaluated were: IL-6, IL-8, IL-10, IL-17, inducible protein (IP)-12p40, IL-1β, TNF- and IFN-. The anti-inflammatory cytokines evaluated were IP-10 and IL-1ra. Concentrations were Community-acquired pneumonia (CAP) is a top ten cause of death in the US over the last 60 years despite the widespread use of antimicrobials.1 Recommended treatment for in-patient CAP is either a β-lactam plus a macrolide or a respiratory quinolone.2 Both regimens cover Streptococcus pneumoniae and atypical pathogens, but macrolides also have immunomodulatory properties. Macrolides, specifically, have the potentially favorable characteristics including (1) anti-inflammatory activity, (2) anti-toxin activity and (3) the tendency to favor apoptosis over necrosis. With the current evidence available, however, it is difficult to independently assess whether the benefit of macrolides is more due to the antimicrobial or immunomodulatory properties. Macrolides have had a known risk of arrhythmia, which prevent it from being given to every patient with CAP “just in case”.3 The work on this topic until now has either addressed the effects macrolides have on the immune system of mice or addressed clinical outcomes in humans without studying immunomodulation. The present study provides both cytokine levels and clinical outcomes in patients hospitalized with CAP.4-6 It evaluated anti-inflammatory activity against antimicrobial activity. The primary objective of this study was to compare serum (1) cytokine levels and neutrophil functions and (2) clinical objectives in hospitalized patients with CAP treated with and without a macrolide. RESULTS Anti-inflammatoryCytokines Among a total of 40 patients, 14 were treated with a macrolide (azithromycin in all cases), while 26 were not. Mean ages were similar between the two groups (52 vs. 60; P=0.178). Demographic data including comorbidities, vaccination status, and severity of disease for the two groups were compared, which showed no marked differences. When comparing laboratory data used to collect the pneumonia severity index and radiological data, there were no statistically significant differences except that a higher proportion of patients who received macrolide treatment had a pleural effusion; (zero vs. 12 (46%); P=0.003). Clinical outcomes for macrolide and non-macrolide patients are in Table 1. P = 0.029 Neutrophil Functions CONCLUSIONS • In conclusion, the present study found lower values for measured cytokines, IL-6, IL-8 and IFN-, after five to seven days from diagnosis of CAP among patients treated with, compared to without a macrolide. There were no differences for neutrophil functions or clinical outcomes between the two groups. • Translational cooperation was successful in this pilot study. * Unless otherwise stated parenthetical value is a proportion; † Defined as ≤ 3 days TCS, time to clinical stability; LOS, length of stay P = 0.021 Pro-inflammatoryCytokines REFERENCES 1 Hoyert DL, Xu J. Deaths: Preliminary data for 2011. National Vital Statistics Reports 2012;61. Mandell LA, Wunderink RG, Anzueto A, Bartlett JG, Campbell GD, Dean NC, Dowell SF, File TM, Jr., Musher DM, Niederman MS, Torres A, Whitney CG, Infectious Diseases Society of A, American Thoracic S. Infectious diseases society of America/American thoracic society consensus guidelines on the management of community-acquired pneumonia in adults. Clin Infect Dis2007;44 Suppl 2:S27-72. Ray WA, Murray KT, Hall K, Arbogast PG, Stein CM. Azithromycin and the risk of cardiovascular death. New Engl Med 2012;366:1881-1890. Arnold FW, Summersgill JT, Lajoie AS, Peyrani P, Marrie TJ, Rossi P, Blasi F, Fernandez P, File TM, Jr., Rello J, Menendez R, Marzoratti L, Luna CM, Ramirez JA, Community-Acquired Pneumonia Organization I. A worldwide perspective of atypical pathogens in community-acquired pneumonia. Am J RespCrit Care Med 2007;175:1086-1093. Restrepo MI, Mortensen EM, Waterer GW, Wunderink RG, Coalson JJ, Anzueto A. Impact of macrolide therapy on mortality for patients with severe sepsis due to pneumonia. Eurresp j 2009;33:153-159. Dwyer R, Ortqvist A, Aufwerber E, HenriquesNormark B, Marrie TJ, Mufson MA, Torres A, Woodhead MA, Alenius M, Kalin M. Addition of a macrolide to a ss-lactam in bacteremic pneumococcal pneumonia. Eur j clin micro infect dis2006;25:518-521. METHODS P = 0.056 This was a prospective study by members of the Community-Acquired Pneumonia Inflammatory Study Group (CAPISG) at the University of Louisville in Louisville, KY from February 14, 2011 until April 14, 2012. Patients with CAP were consented to have their blood drawn for neutrophil function and cytokine





















