Emergency contraception
Emergency contraception. Sajid Khan GPST2. Emergency contraception. Methods of emergency contraception Indications for use of emergency contraception Methods of action Clinical Effectiveness Consultation. Emergency Contraception.

Emergency contraception
E N D
Presentation Transcript
Emergency contraception Sajid Khan GPST2
Emergency contraception • Methods of emergency contraception • Indications for use of emergency contraception • Methods of action • Clinical Effectiveness • Consultation
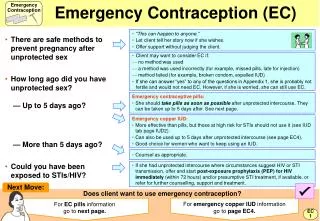
Emergency Contraception • Emergency contraception- (the morning-after pill) refers to the use of drugs or a device as an emergency measure to prevent pregnancy. • Given to • Women who have had recent unprotected sexual intercourse • Failure in another method of contraception
Methods of emergency contraception • Levonorgestrel, LNG (oral pill) • “Levonelle 1500, Levonelle one step” • Ulipristal/UPA • “ellaOne” (oral pill) • Copper Intrauterine Device
When is EC needed? • Missed cocp • Late POP ( >27 hrs for conventional POP,>36 hours for cerazette) • Late depot • Condom not used/ condom accident • IUD removal, expulsion, lost threads • Enzyme inducing drugs and failure to use extra precautions
Levonorgestrel, LNG (oral pill)“Levonelle” • Levonelle 1500 (pom); Levonelle one step; • A progesterone; single 1.5mg dose • Licensed for use up to 72 hours after UPSI or contraceptive failure • Mechanism of action: works primarily by inhibition of ovulation. LNG appears to prevent follicular rupture or cause luteal dysfunction. • LNG taken prior to the LH surge has been shown to result in ovulatory dysfunction in the subsequent 5 days. • Inhibit ovulation for 5–7 days, by which time any sperm in the reproductive tract will have become non-viable.
Ulipristal/UPA “ellaOne” (oral pill) • A selective progesterone receptor modulator; single dose 30 mg. • Licensed for use up to 120 hours after UPSI or contraceptive failure. • Cost £16.95 • Mechanism of action: ; delays LH surge and has effect on follicular rupture; • Affects hormonal contraception for a short while afterwards(extra barrier protection cocp 14 days, pop 9 days)
Copper IUD • Copper IUD; can be used up to 5 days following first UPSI in cycle or within 5 days from the earliest estimated day of ovulation. • Mechanism of action: copper toxic to sperm and ovum; primarily inhibits fertilisation (and implantation) • Effectiveness >99% at any time of cycle
How effective are they? • IUD >99% effective • LNG up to 95% within 24 hrs • up to 85% within 25-48 hrs • up to 58% within 49-72 hrs • UPA at least as effective as LNG up to 120 hours
Evidence LNG vs UPA • Ulipristalacetate versus levonorgestrel for emergency contraception: a randomised non-inferiority trial and meta-analysis. • Glasier AF et al Lancet. 2010 • Two randomised controlled trials • 1696 women received emergency contraception within 72 h of sexual intercourse (ulipristal acetate, n=844; levonorgestrel, n=852). There were 15 pregnancies in the ulipristal acetate group (1.8%,) and 22 in the levonorgestrel group (2.6%). • In 203 women who received emergency contraception between 72 h and 120 h after sexual intercourse, there were three pregnancies, all of which were in the levonorgestrel group. • Pregnancy rate lower in UPA than LNG
Emergency contraception: Consultation • Date of LMP; • Time since UPSI • Previous UPSI this cycle? • EC used this cycle? • Discussed oral method v IUD? • Ongoing contraception discussed? • Health promotion • Need STI screen? • Given leaflets for contraception • Condoms offered if needed? • Advised PT in 3weeks if no period