Medicaid Expansion Status
220 likes | 434 Vues
Medicaid Expansion Status. Medicaid Opportunities & Challenges Task Force April 24, 2013 Jeff Bechtel, Senior Consultant Jennifer Jordan, Senior Consultant. Agenda for Today’s Briefing. Overview of State Expansion Status Medicaid Expansion Debate Arguments for Expansion

Medicaid Expansion Status
E N D
Presentation Transcript
Medicaid Expansion Status Medicaid Opportunities & Challenges Task Force April 24, 2013 Jeff Bechtel, Senior Consultant Jennifer Jordan, Senior Consultant
Agenda for Today’s Briefing • Overview of State Expansion Status • Medicaid Expansion Debate • Arguments for Expansion • Arguments against Expansion • State Approaches
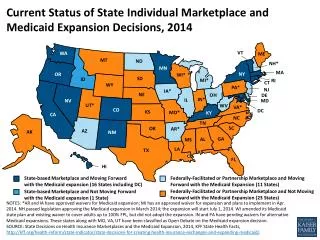
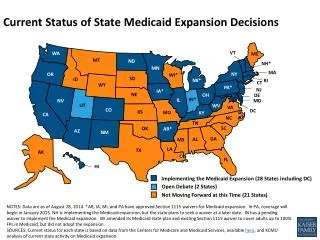
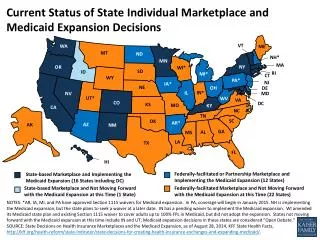
Where States Stand Now on Medicaid Expansion Some Governors have already signaled their intent to either opt-in or opt-out of the expansion. However, many states have not taken a definitive position. In some cases, Governors and state legislative leaders have offered differing opinions. Here is a preliminary snapshot of where states stand based on news reports and statements by Governors.* • Executive Status: • Proposing expansion: 27 • Not proposing expansion: 19 • Weighing options: 4 *Kaiser Family Foundation analysis as of April 16, 2013. Subject to change.
Medicaid Expansion Debate • Major stakeholders have advocated strongly for states to opt for ACA Medicaid eligibility expansion. • These stakeholders include hospitals and health systems, physicians, community health centers, and consumer and patient advocates. • Stakeholders have raised a number of arguments in favor of their state opting to expand Medicaid eligibility. • The following slides include a sampling of 10 arguments that have been raised by stakeholders in favor of Medicaid expansion and 10 arguments that have been raised opposing Medicaid expansion. • These are provided for illustrative purposes without comment on their relative merits, counter arguments, or appropriateness for any given state. • Various other arguments – pro and con – have been made.
Ten Arguments for Medicaid Expansion • Good Financial Deal for the State: • The enhanced federal match of 100% for three years for services, transitioning downwards to 90% by 2020, is a good financial deal for states. • This is far higher than 50% to 77% states receive for rest of Medicaid benefit spending. • States have flexibility in deciding to expand Medicaid. It is not “now or never” and states could choose to back out. • Economic Impact: • The additional federal funding will lead to new jobs, tax revenues, and other economic benefits. • Many states will see well over $1 billion in new federal funds annually.
Ten Arguments for Medicaid Expansion (cont’d) • Impact on Hospitals: • Hospitals already face serious financial pressures as a result of uncompensated care and payment cuts. This is unsustainable and threatens access to care for everyone. • ACA Payment Cuts: • To help pay for the federal cost of Medicaid expansion, the ACA made significant Medicare rate cuts and will cut Medicaid and Medicare payments for uncompensated care costs (disproportionate share hospital payments). (Note: CMS has delayed cuts for one year). • Theses cuts were predicated on the fact that uninsured rates would decline by about 50%, with most newly insured being covered through Medicaid. • Hospitals and other providers face years of big payment cuts without the corresponding increase in coverage on the uninsured.
Ten Arguments for Medicaid Expansion (cont’d) • Health Benefits of Coverage: • Insured individuals are more likely to receive needed care and preventive screens, thereby lowering future medical costs. It also impacts employability and thus workforce competitiveness. • State Business Environment: • Non-expansion will make a state less competitive for employers. • Employers in non-expansion states must continue to absorb cost shifting and thus higher premiums, making them less competitive. Businesses will “vote with their feet” and relocate to expansion states. • Non-expansion states may experience workforce issues. Employees may move to states that expand Medicaid to obtain health insurance.
Ten Arguments for Medicaid Expansion (cont’d) • Fairness to State Taxpayers: • As federal taxpayers, residents of non-expansion states will subsidize the residents, employers, and providers of expansion states. • Disparities: • The Medicaid expansion population is disproportionately minority. • Expansion is needed to help reduce racial, ethnic, and geographic disparities in healthcare access and quality.
Ten Arguments for Medicaid Expansion (cont’d) • Medicaid Provides Cost-Effective Coverage: • The Medicaid expansion is a cost-effective way to provide coverage. • Medicaid’s administrative and PMPM costs are much lower than commercial insurance. • Woodwork Effect Will Happen Anyway: • Medicaid expansion won’t impact other Medicaid program growth (i.e. the Woodwork effect), which will happen in any event.
Ten Arguments Against Medicaid Expansion 1. Expansion of Broken, Entitlement Program: • Medicaid is fiscally unsustainable and needs substantial, fundamental reform, not expansion. 2. Risk of Bait and Switch in Federal Matching Funds: • Federal government spending (Medicaid and Medicare spending in particular) is unsustainable. • The federal government simply does not have the money to pay for the enhanced matching funds offered in ACA. • Once a state opts in, it will be politically difficult to later opt out when the feds cut back on funding.
Ten Arguments Against Medicaid Expansion (cont’d) 3. Large State Budget Impact in Out Years: • Given the number of new adult enrollees even a state match of 5% or 10 % would be a major new cost to the state budget. 4. Woodwork Effect Will Increase Medicaid Enrollment: • The woodwork effect will be much higher with the presence of Medicaid expansion. • Costs of the woodwork population – already eligible under pre-ACA policies but not enrolled – will be paid for using the standard, lower federal match rate and correspondingly higher state share – with a hit to state budgets.
Ten Arguments Against Medicaid Expansion (cont’d) 5. Crowd Out of Private Insurance: • Not everyone newly enrolled in Medicaid – whether through the ACA Medicaid eligibility expansion option or the woodwork effect – will be newly insured. • According to CBO projections, about 30% of those new to the Medicaid rolls will already have private health insurance coverage (i.e. crowd out population). • Higher Priority State Reforms: • States have other, higher priorities. 7. A Taxpayer is a Taxpayer, Whether Federal or State: • State officials should be responsible and not hurt taxpayers by accepting debt-financed money for Medicaid expansion.
Ten Arguments Against Medicaid Expansion (cont’d) 8. Provider Capacity Will be Stretched in 2014: • Current provider capacity – especially the capacity of primary care physicians, hospital emergency departments, and safety net providers in general – will be stretched in 2014 due to Health Insurance Exchange enrollment. 9. Availability of Coverage through Health Insurance Exchanges, Opportunity to Reduce Current Medicaid Eligibility: • A significant percentage of the target population for Medicaid expansion are citizens who fall between 100% and 138% of FPL and therefore will have access to federally subsidized premiums and cost sharing in the Health Insurance Exchange.
Ten Arguments Against Medicaid Expansion (cont’d) 10. Unanswered Questions, Unclear Impact of ACA: • There are still significant unanswered questions relating to the Medicaid expansion, and the impact of the ACA on the insurance marketplace is unclear. • Decisions on this issue should be delayed until the consequences of expansion are clear.
State Approaches • As states have debated and evaluated the expansion, several Governors have sought to change the nature of the expansion and the operation of Medicaid in their states. • The federal Department of Health and Humans Services appears open to some flexibility, within the confines of federal law and with consideration to the precedent-setting nature of each individual decision. • A number of strategies have been laid out. Each strategy is based on each state’s individual program context (current eligibility levels, benefit design and service delivery model). • These strategies are preliminary approaches; it is unclear if they will be adopted in one or more states, or approved by CMS. 18
Premium Subsidy (“Arkansas Approach”) Concept Overview/Requirements: • All newly eligible enroll in private coverage through Exchange • 100% FMAP on costs of Exchange premiums for expansion population for the first three years • Expansion population still entitled to the Medicaid benefit guarantees • State must offer wraparound coverage for Medicaid benefits no covered in Exchange • State must meet cost-sharing protections Considerations: • Cost of coverage - Purchasing a private plan through the Exchange vs. Medicaid coverage • Provider reimbursement rates – Medicaid vs. Commercial • Opportunity to obtain pharmacy rebates • Actuarial impact of the Medicaid expansion group on overall Exchange premiums. • Loss of state control (Medicaid administered by State, Exchange by federal government) • Limited number of CMS “Pilots”
Implement Expansion with Conditions Concept Overview: • Medicaid expansion only if certain conditions are met: • Approval conditional on meeting specific program reforms • Mandatory review of the program if its expenses were to skyrocket • Requirement that the state withdraw if the federal government fails to fund expansion as promised (“circuit breaker”) • Authorization sunset timed to the end of 100% FMAP Considerations: • Delay in program implementation cuts into three-year 100% FMAP period • Political feasibility of opting out once expansion is implemented
Hybrid Approach (“Wisconsin Model”) Concept Overview: • Allow extremely poor childless adults (below 100% FPL) to enroll in Medicaid • Shift consumers above 100% FPL (who are currently in Medicaid) into federally-subsidized Exchange Considerations: • CMS approval- Approach appears to be a non-starter with CMS in that partial expansion is prohibited • Wisconsin already covers, through a CMS waiver, adults up to 138% of FPL • Premiums and higher cost-sharing for individuals 100% - 138% FPL in Exchange
For More Information • Sellers Dorsey • www.sellersdorsey.com • Jeff Bechtel, JD • Senior Consultant • Sellers Dorsey • 717.712.6247 • jbechtel@sellersdorsey.com • Jennifer Jordan • Senior Consultant • Sellers Dorsey • 215.279.9739 • jjordan@sellersdorsey.com