Download
1 / 45
560 likes | 1.35k Vues
Acute Respiratory Distress Syndrome. Susie Gerik, MD Children’s Special Services. Objectives. Describe features of ARDS List possible inciting conditions Describe pathophysiology Discuss treatment strategies Address morbidity and mortality. History. Described by William Osler in 1800

E N D
Acute Respiratory Distress Syndrome Susie Gerik, MD Children’s Special Services
Objectives • Describe features of ARDS • List possible inciting conditions • Describe pathophysiology • Discuss treatment strategies • Address morbidity and mortality
History • Described by William Osler in 1800 • Asbaugh et al., Lancet 1967 • Observed in adults and children
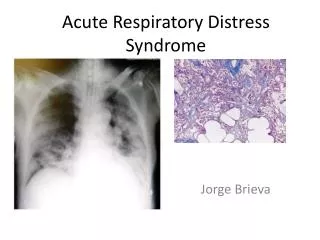
Definition • Condition characterized by acute inflammatory lung injury resulting in widespread pulmonary edema as a result of increased alveolar capillary permeability and epithelial destruction.
Features • Acute respiratory distress • Cyanosis refractory to oxygen • Decreased lung compliance • Diffuse infiltrates on CXR
1988 Lung Injury Score • PEEP • PaO2/FIO2 ratio • Static lung compliance • Degree of infiltrates
1994 Consensus • Acute onset • PaO2/FIO2 < 200 • Bilateral infiltrates • PCWP < 18
1994 Consensus • Two categories: • Acute lung injury: PaO2/FIO2 ratio < 300 • ARDS: PaO2/FIO2 < 200
Incidence • Acute Lung Injury: 17.9/100,000 • ARDS: 13.5/100,000 • ~1% of all PICU admissions
Causes • Shock • Aspiration • Trauma • Infections • Inhaled fumes • Drugs and poisons • Miscellaneous
Ventilator-induced Lung Injury • Barotrauma • large lung volumes • Atalectrauma • shear forces • Biotrauma • activation of effector cells to release mediators
Indirect Injury • Sepsis syndrome • Severe nonthoracic trauma • Post cardiopulmonary bypass • Post hemodialysis • Disseminated intravascular coagulation • Pancreatitis • Antiphospholipid syndromes
Pathogenesis • Inflammatory mediators • damage to microvascular endothelium • damage to alveolar epithelium • increased alveolar permeability • accumulation of alveolar edema fluid
Pathogenesis • Neutrophils and macrophages • Complement • Cytokines • Platelet activating factor • Eicosanoids • Free radicals
Pathophysiology • Abnormalities in gas exchange • Abnormalities in oxygen delivery and consumption • Abnormalities in cardiopulmonary interactions • Multiple organ involvement
Gas Exchange - Hypoxemia • Increased capillary permeability • Interstitial and alveolar exudate • Intrapulmonary shunting • Reduced ventilation-perfusion matching • Diffusion defect with right to left shunt
Pulmonary Mechanics • Reduced lung volume (FRC) • Reduced lung compliance • Impaired function of surfactant
Pathologic Flow • Uncoupling of oxidative dependency • Oxygen utilization by non-ATP producing oxidase systems • Increased diffusion distance for O2 between capillary and alveolus
Cardiopulmonary Interactions • Pulmonary hypertension -> increased RV afterload • High PEEP -> decreased preload • Results in decreased cardiac output
Non-pulmonary Abnormalities • Multi-organ system failure • Bio-trauma • Pathologic oxygen-supply dependency
Max O2 extraction VO2 Critical DO2 DO2 Normal VO2 = DO2 X O2ER Substrate utilization Max O2 extraction VO2 Critical DO2 DO2 Septic Shock/ARDS Abnormal Flow Dependency
Acute, Exudative Phase • Rapid respiratory failure after trigger • Diffuse alveolar damage with inflammatory infiltrate • Hyaline membrane formation • Capillary injury • Protein-rich edema fluid in alveoli • Disruption of alveolar epithelium
Subacute, Proliferative Phase • Persistent hypoxemia • Development of hypercarbia • Fibrosing alveolitis • Further decrease in pulmonary compliance • Pulmonary hypertension
Chronic Phase • Obliteration of alveolar and bronchiolar spaces and pulmonary capillaries
Recovery Phase • Gradual resolution of hypoxemia • Improved lung compliance • Resolution of CXR abnormalities
Goals of Treatment • Optimize gas exchange and O2 delivery • Minimize ventilator-induced lung injury • Treat etiology • Avoid multisystem organ failure
Treatment: Respiratory Support • Mechanical ventilation • High frequency ventilation • ECMO • Nitric oxide • Liquid ventilation • Exogenous surfactant
Treatment: Monitoring • Respiratory • Hemodynamic • Metabolic • Infections • Fluid/electrolytes
Optimize VO2/D02 Relationship • DO2 • hemoglobin • mechanical ventilation • oxygen (PEEP) • VO2 • preload • afterload • contractility
Ventilation Strategies • Oxygen • PEEP • Inverse I:E ratio • Lower TV • Prone position
PEEP • Displaces edema fluid into interstitium • Decreases atalectasis • Decreases right to left shunt • Improves compliance • Improves oxygenation
Nitric Oxide • Pulmonary vasodilation • Selectively improves perfusion of ventilated areas • Reduces intrapulmonary shunting • Improves arterial oxygenation • No systemic hemodynamic effects
Prone Position • Improved gas exchange • Uniform alveolar ventilation • Recruitment of segments in dorsal region • Improved postural drainage • Redistribution of perfusion away from edematous, dependent regions
High Frequency Ventilation • Raises MAP • Recruits lung volume • Small changes in TV • Impedes venous return
Liquid Ventilation • Perflubron • 20x O2 and 30x CO2 solubility • Heavier than water • Higher spreading coefficient • Improved compliance and gas exchange
Mortality • 40-60% • Multiorgan failure/sepsis • Decreasing because of better vetilatory strategies and earlier recognition and treatment
Iatrogenic Contributors to Morbidity/Mortality • Inadequate nutrition • Fluid overload • Inappropriate sedation • Neuromuscular blocking agents • Complications from medical procedures • Medical errors
Prognostic Factors • Underlying medical condition • Presence of multiorgan failure • Severity of illness