HERD, Nepal
The development and implementation of supervision and patient support approach in Drug Resistant TB management programme in Nepal 17,Baishakh, 2071 (30 April 2014) g]kfn ;/sf/ :jf:Yo tyf hg;+Vof dGqfno. HERD, Nepal. Aim:


HERD, Nepal
E N D
Presentation Transcript
The development and implementation of supervision and patient support approach in Drug Resistant TB management programme in Nepal 17,Baishakh, 2071 (30 April 2014) g]kfn ;/sf/ :jf:Yo tyf hg;+Vof dGqfno HERD, Nepal
Aim: To contribute for effective management of DR-TB case through development and implementation of a locally feasible supervision and patient support approach in the existing DR-TB management programme, which is patient friendly and feasible to scale-up. Study Design: Randomised Control Trial Study site: Selected DR-TB treatment centres and sub centres (sites yet to be randomised and selected)
Phases of the study: • Phase 1: Exploratory study to identify the needs of the patients and development of supervision and patient support package; • Phase 2: Implementation of the package • Phase 3: Follow up for 20 months and evaluation of the effectiveness of the package. Current status of the Project: Draft of the package designed based on findings and review of evidence. Paper on findings of the study in the process of write up.
Way forward: • Design Workshop: Discussion and finalization of the intervention in discussion with the relevant stakeholders. • Development of the required IEC materials based on the intervention developed in coordination with the stakeholders. • Implementation of the intervention and follow up in the selected sites.
Stage 1 • Qualitative study in different parts of the country • Conducted in depth interviews with patients (n=11), family members (n=4) and a few health workers (n=3). • Focus group discussions with patients and family members (3)
Key Findings • Various subgroups or types of patients exist within the umbrella of MDR TB patients. • Needs of the various groups or types of the patients varied • The need of patients varies depending on the phase or time of completion of treatment. • Some groups of patients were identified as the most vulnerable ones in terms of the support needed, particularly women and men who had relocated
Our major Learning from the study: • Where some kind of similar interventions is needed for all the MDR TB patients, some aspects need be individualized and tailored as the need of various patient is different.
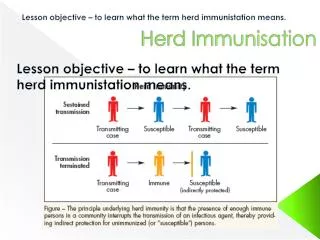
Information on infection control • Patients have incomplete or fragmented information about the various ways on infection control. • Some misconceptions exist which often leads to self isolation in order to avoid transmission to their loved ones. • Most of the patients seemed not very clear about the time period when they remain extremely infectious and relate the concept of intensive and continuous phases with application of injections
I was scared as TB can get transmitted through breath as I used to stay with my family most of the time. Till the time my result was negative, I used to stay away from my friends and was depressed. I was a bit relieved when my reports showed negative but at the same time fear was there that the report may be positive later
Information on Drug side effects • Physical side effects commonly observed by most of the patients • Inadequate information on ways of dealing with the side effects • Patients pointed out prior information on the potential side effects of drugs and its management would help reduce their worry • Patients unable to recognize the psychological side effects and often seek help for the physical ones. (educate them to be able to identify the psychological problem)
Information on nutrition • Patient are aware of the nutrition needs. However, affordability remains a question • Need for information on use of the locally available food to meet their dietary requirements.
Sources of knowledge • Dots incharge are the sources of knowledge to majority of them • Unavailability of any IEC materials specific to MDR (posters or leaflets)
Impact of the disease • Physical impact • Social relation (self isolation, stigma, family relationships-particularly women) • Relocation • Livelihood (inability to earn) (treatment Vs work) • Psychologically: fear, hopelessness, loosing the desire to survive, demoralized, depression • Financial and other difficulties to the family members • Far location of the treatment centres.
Psychological aspect I have 90% chances of dying. There is only 10% chance that I'll survive. That is how I feel because I cannot even go to the toilet. I need support. When I eat, I immediately throw up. I take my medicines and I immediately throw up. I don't feel like looking at anything.” (III interview 1) Before I used to feel that it is no big deal to have TB but now since I have it, I feel there is no chance to get this cured.” (I interview 4)
MDR causes various psychological affects to the patients • Need of the kinds of psychological support is different. • Women are the most vulnerable groups: forced out of their houses by their family members after being infected • Patients who have had to relocate also require psychological support • Hostel patients: support they are receiving is inadequate, need for group support
Financial issues • Financial hardships faced by all. • Most badly affected are the relocated patients and the unsupported women. • Difficulty in managing work and the treatment especially women who have to sustain themselves.
Most of the patients irrespective of their area, location, treatment duration and socioeconomic conditions reflected knowledge and awareness about provision of monthly financial incentive of Rs 1500 to MDR patients undergoing treatment. • Regular and timely dis imbursement of the incentives is a concern for patients • Those managing work and treatment face difficulty to go collect the incentive from the centres. • Most of the patients use the financial incentive for transport rather than food and nutrition (except the hostel patients)
Health facility related issues • Far location of the treatment centre making the treatment difficult. Especially for the poor patients as the transportation would cost them money. • Issue of privacy: particularly women as they found it uncomfortable taking injection in open area where people could see them. • Confidentiality: Patient of all groups didn’t want to be seen by others in the centre.
Health workers related: • Behavior of health workers has a great effect on adherence and treatment of the MDR-TB patients. • Most of the patients perceived dots incharge to be busy and stated they didn’t want to disturb them when small problem arise.
A few of the patients and their family members mentioned the need of a counselor with technical expertise (MDR) separately in the centres for providing advice and or counseling • Most of the patients weren't aware about the TB-HIV co infection and mentioned they did not know if they have been tested for HIV
Summary of the Perceived gaps by patients Need for: • Information on various aspects of the disease during the treatment time • Psychological support • Social support :Involving family /relatives in the counseling or treatment process • Stigma • Increased financial support
Counselling using IEC materials Psychosocial support Information Our intervention focus
Proposed Intervention • 6 Scheduled counseling visits with the DOTS incharge at different time of the treatment duration • These visits to be recorded using forms that’s will be developed • Use of IEC materials to facilitate counseling • Psychosocial support at various visits according to the need of the patient. • DOTS incharge will be trained for providing counseling
Visits Schedule ContinuationPhase Intensive Phase Sputumconversion Visit 6 Last week of treatment Visit 1 Day 1 Visit 2 1 month Visit 3 3 month Visit 4 8 months Visit 5 18 month Treatment time (20 months)
Visit 1: Day 1 IEC materails used: Flipbook and leaflet/posters AIM: Give basic information to the patient about the disease, treatment duration and on the adherence of treatment More emphasis on providing psychological support Caution: Not much information about the various side effects of the medicine as we don’t want to scare them
Counseling to the patients covering the following: • Emphasis on information from HW • About MDR TB disease • Different tests need to be done before starting treatment • Mode of transmission • Infection control/Deal misconception • Importance of drug adherence • Treatment and treatment duration • Importance of nutrition(Generic) • Side effects (general) • PSYCHOLOGICAL COUNSELLING BASED ON THEIR NEED/LEVEL • Follow up examination
If the patient has brought his Family Member • HW to give information to family member about the following things in addition to the above: • Importance of family member role and how can they support in the treatment-What they should do? • Reminder for medicine • Side effect of treatment • Importance of them giving psychosocial support to the family member • Give leaflet to family member • Nutrition and its supplements • Ask them to accompany the patient(as much as possible) if not at least 6 months follow up
Visit 2: 1 month • IEC materails used: Flipbook/leaflet/posters • Aim: To reinforce the information given in the 1st visit • Provide psychological support as required
Counseling to emphasize on: • Importance of adherence • Importance of Nutrition and its locally available supplements • Side effects and ways to cope or deal with it) • Infection control measures • PSYCHOLOGICAL COUNSELLING BASED ON THEIR NEEDS • Follow up examination
Visit 3: 3 months • AIM: check if the patient has been experiencing any side effect • Give him more information about the drug side effects and the ways to deal with it • Reemphasize the importance of treatment adherence
Checking for any side effects • If yes, side effect management • Importance of adherence • Nutrition importance and substitutes • PSYCHOLOGICAL COUNSELLING BASED ON NEED OF PATIENTS • Remind patients to bring their family member along in the next schedule visit (8 month)
Visit 4: 8 months • AIM: Motivate patient for treatment adherence • More on psychological counseling based on their need and report after the sputum conversion test
If sputum is negative • Emphasize on nutrition importance and substitutes • Importance on not stopping to take medicine • If sputum is positive PSYCHOLOGICAL COUNSELLING –need to motivate the patient and reassurance Emphasize on importance of continuing the treatment
If accompanied by family members: • Talk to family members about treatment regimen • side effect management • Family members to be explained well about about their relatives' condition(physical + psychological) • Nutrition and their supplements
Visit 5: 18 months • PSYCHOLOGICAL COUNSELLING BASED ON NEED • Motivational counseling
Visit 6: last week of the treatment • Motivational counseling • Preparation to get back to normal life
Points to note • Keep record of the number of informal (other than the scheduled visits) sessions with patients • If a patient’s intensive phase is prolonged note down the duration of extension and the number of informal counselling during that time
Few points to think about • Is it feasible of having a support group initiated and facilitated by the dots incharge once the patient is in continuation phase?? • Feasibility of giving time for counseling to the patients