Download
1 / 30
310 likes | 835 Vues
OBSTETRICS/FEMAL PELVIS : OB 5. THE PRENATAL DIAGNOSIS OF CONGENITAL CYSTIC ADENOMATOID MALFORMATION. S. FEKIH AHMED 1 , MA. JELLALI 1* , S. BELHASSEN 2 , S. MOSBAHI 2 , A. ZRIG 1 , W. MNARI 1 , L. SAHNOUN 2 , K. MAAZOUN 2 , A. KSIAA 2 , S. HIDOURI 2 , M. MEKKI 2 , A. NOURI 2 , M. GOLLI 1

E N D
OBSTETRICS/FEMAL PELVIS : OB 5 THE PRENATAL DIAGNOSIS OF CONGENITAL CYSTIC ADENOMATOID MALFORMATION S. FEKIH AHMED1, MA. JELLALI1*, S. BELHASSEN2, S. MOSBAHI2, A. ZRIG1, W. MNARI1, L. SAHNOUN2, K. MAAZOUN2, A. KSIAA2, S. HIDOURI2, M. MEKKI2, A. NOURI2, M. GOLLI1 1Radiology service, FB Hospital, 1st June street, 5000 Monastir, Tunisia. 2Pediatric surgery service, FB Hospital, 1st June street, 5000 Monastir, Tunisia. *jellalimedali@yahoo.fr
Objectives The objectives of this study weres to show the several sonographic appearance of congenital cystic adenomatoid malformation (CCAM) and to demonstrate the importance of US in the prenatal diagnosis .
Materials and methods • The medical records of 4 patients with pathologically proven congenital cystic adenomatoid malformations were retrospectively reviewed . • These cases of CCAM werediagnosed in antenatal in Monastir hospitalduring the periodfrom 1996 to 2009 . • The Stocker classification wasused .
1st observation • female • Prenatal Sonography at 28 weeks’gestationnal age : • Cysts at the right lung ( inferior lobe ) • Hydramniosis and a mild compression of the mediastinum .
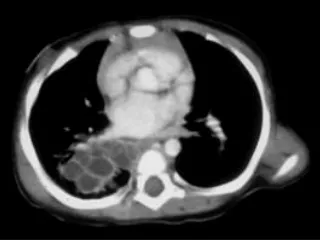
4 months: COUGH • Chest radiograph:Anteroposterior radiograph shows • hyperlucent right lung with mass effect causing deviation of the • mediastinum towards the left • hemithorax. . CT : multicystic mass measuring 5 cm in the right lower lobe . The cysts have variable size, thin wall , contain air and cause mediastinal shift .
Inferior right lobectomy • 2cm –cystic – bilocular mass • satisfying follow-up .
2nd observation Sex : female Prenatal Sonography at 36 weeks’ gestationnal age : intra thoracic cystic mass in the right para vertébral région ,
At the age of 7 months : Pneumonia A 4 cm-size cyst with air-fluid level , it’s located in the lower part of the right lung ; it’s associated with homolateral pleural effusion .
CT : Well circumscribed cyst containing air-fluid level in the right lower lobe , there are no enhancement . • At the age of 8months : • right postero-lateral thoracotomy • inferior right lobectomy
3rd observation Male , prenatal sonography at 30 weeks’ GA : Intrathoracic cyst measuring 3 cm . 8 months : cough , well cicumscribed hyperlucent lesion in the right lung . CT : Right Lower lobe : Multicystic mass with air in cysts .
Superior right lobectomy !! CCAM type I of Stocker
4th observation Male , prenatal sonography at 35 weeks’ GA :cyst in the right lung . At birth : respiratory distress Chest radiograph : hyperlucent right lung . There is mediaslinal shift to the left.
Operated at the age of 5 days : inferior right lobectomy . Satisfying follow-up .
RESULTS • They were 2girls and 2 boys. • Prenatal sonographic examination was always performed between 28 and 36 weeks’ gestational age. It showed cysts that measure in average 24 mm. They were CCAM type I of STOCKER . • They were in the right lung in all cases. It was always a single lobe disease . • All the pregnancies intended to continue resulted in live birth(100 % survival rate ) .They were delivered at term . • All patients were asymptomatic at birth . • They became symptomatic respectively at the age of 1, 4 and 7 months; one patient was still asymptomatic . • All children underwent surgery with satisfying follow up.
DISCUSSION • Congenital cystic adenomatoid malformation(CCAM) was briefly described by Stoerk in 1897 and later in detail by Ch'in and Tang. Since the initial description in a 1-month-old infant with respiratory distress and anasarca, many cases have been described . • It accounts for approximately 95 percent of congenital cystic lung diseases. It usually presents in infancy with respiratory distress secondary to a space-occupying lesion that compromises normal lung tissue. • Patients with congenital cystic adenomatoid malformations are not all symptomatic at birth, with delayed presentation and diagnosis occurring in adulthood.
Male subjects are affected as often as female subjects. In our study , it was 2female/2 male . • The left lung is involved as often as the right with single lobe disease observed four times more often than multilobe disease.. • It is unilateral in 98% of the cases . • In our cases it was always a single lobe disease in the right lung .
Pathology : • Cystic adenomatoid malformation of the lung is a hamartomatous lesion that results from cessation of normal bronchiolar maturation with proliferation of mesenchymal elements in the lung. • These hamartomatous lesions have no preference for sex or location within the lung. • Spontaneous regression was described , it is no higher than 6%.I n our study , all lesion didn’t regress . • Stocker et al (1977) described three types, on several criteria but basically on the size of the cysts.
Stocker classification( Hum Pathol1977) : • Type I (50% ): contains well-differentiated bronchial components but no cartilage. It contains large cysts (greater than 2 cm) seen in sonography . • Type II (40% ): they are thought to occur due to an earlier arrest of normal lung development. Numerous small cysts of uniform size between 5 mm and 2 cm . • Type III (10 % ) :they are thought to be caused by an even earlier embryologic insult.These lesions show minimal differentiation between mesenchymal and epithelial structures and contain microscopic cysts (< 5mm ) that result in a US appearance of a large bulky echogenic mass. Microcysts are not seen in imaging .
Type I : excellent prognosis ,as in our cases. • Type II and III : poor prognosis (respiratory insufficiency ,marked pulmonary hypoplasia with the type III… )
Associated malformation : • Reported in 18 %of patients: renal agenesis and cardiac anomalies are predominating . • 89 % of patients with CCAM present with mediastinal shifts, 68% with polyhydramnios, 62% with ascites, and 62% with hydrops in the prenatal period. • 25 % of patients, most commonly those with type II disease, have associated abnormalities of the kidneys and gastrointestinal tract as well as chromosomal abnormalities . • In our study , there are a case of hydramnios and two cases of mediastinal shift. • There are no associated malformation .
Prenatal sonographic diagnosis : • Prenatal sonographic diagnosis of CCAM of the lung has been described in the medical literature since the 1980s. • Before the advent of prenatal sonography, CCAM were diagnosed primarily in symptomatic children or in the occasional asymptomatic child in whom the lesion was detected as an incidental finding on a radiograph.
CCAM canbeidentified by US since 17 weeks GA , generallybetween 17 and 24 weeks GA • In ourstudy , US examinationswererelativelylatedonebetween 28 -36 weeks’GA . • UltrasonographicFindings : o Echogenic fetal lung mass ; cysts in type I and II o Mediastinal shift o Fetal hydrops may occur o Polyhydramniosmayoccur oCCAM type 2 may become less apparent on serial fetalultrasound.
Adzik and Al (J pediatrsurg 1985) • proposed a sonographic classification in which differenciated two subgroups based on the sonographic appearance of the cysts: • Macrocystic with cysts ≥ 5mm . It appears as an echogenic mass with scattered cystic areas . Stocker I and II . • Microcystic with cysts < 5mm. It appears as a hyperechoic mass , microcysts are not seen by US Stocker III . • Imaging appearance depends upon size of cysts.
Prenatal sonography has changed the spectrum of patients identified CCAM • It can identify a patient population with a developmental lung anomaly who may or may not be symptomatic at birth. • In both groups, early diagnosis allows prenatal counseling, possible fetal intervention, and birth planning.
Fœtal MRI : Used if doubtful prenatal diagnosis . • T1Wl o lsointense lesion • T2WI o Hyperintense mass o Often demonstrates mediastinal shift o Compression of adjacent lung o May be associated with fetal hydrops
Cystic adenoid malformation (33 GA): Coronal T2- weighted image S. Launay,JGynecolObstetBiolReprod , 2003
Differential diagnoses: • The major differential diagnoses include diaphragmatic hernia, penicardialteratoma,andbronchopulmonary sequestration • CongenitaldiaphragmaticherniaCDH : • May coexistwith CCAM. • Appears as multicystic, air-containing mass • Appearance can change in position with CDHover serial films . • Position of support apparatus altered with CDH (i.e.nasogastric (NG) tube, umbilical venous catheter(UVC) can help with diagnosis • Lack of bowel gas in abdomen
Pericardial teratoma: • Echogenic solid mass that displaces the heart and usually produces hydrops fetalis. • The mass appears to arise from the area of the pericardium. • Bronchopulmonary sequestration: • Echogenic mass with a spherical shape or conical or triangular shape .it is usually well-defined, homogeneous and echogenic structure located in the left lower lobe .
CONCLUSION • Prenatal sonography provides the radiologist means to identify congenital cystic adenomatoid malformations in a population of infants who are asymptomatic at birth. • Early diagnosis allows prenatal counseling, possible fetal intervention, and birth planning.
REFERENCES • B A Carroll. Ultrasound case of the day . RadioGraphics 1991; 11:1140-1142 . • A Harper . Prenataldiagnosis of cystic adenomatoid malformation of the lung in a twinpregnancy. The Ulster Medical Journal 1992;61:102-105. • M MCloutier, D A Schaeffer and D Hight.Congenitalcystic adenomatoid malformation. Chest 1993;103;761-764 . • A M.Hubbard, N S Adzick .congenitalchestlesion:diagnosis and characterizationwithprenatal MR imaging .Radiology 1999;212:43-48 . • G Monni,DPaladini. Prenatalultrasounddiagnosis of congenitalcystic adenomatoid malformation of the lung : a report of 26cases and review of literature . Ultrasoundobstetgynecol 2000;16:159-162 . • K W Marshall.C E Blane .Congenital Cystic Adenomatoid Malformation: Impact of Prenatal Diagnosis and Changing Strategies in the Treatment of the Asymptomatic Patient .AJR 2000;175:1551–1554 . • S Launay, V Cuilleret . Applications de l’imagerie par résonance magnétique en obstétrique. J GynecolObstetBiolReprod 2003 ; 32 : 205-220. • Y Robert, V Cuilleret . IRM thoracique fœtale. EMC Radiodiagnostic - Coeur-Poumon 2005; 5 :32-497-A-10 . • M B Daudruy , D Eurin .apport de l’échographie avec Doppler couleur et pulsédans les malformations pulmonaires du foetus .J Radiol 2007;88:269-276 .