Download

1 / 18
180 likes | 208 Vues
Learn about nephrons, the functional units of the kidneys, their structure including glomerulus, tubules, and juxtaglomerular apparatus. Discover their role in urine production and regulation of body fluids. Explore pathologies affecting nephrons.

E N D
URINARY TRACT – II Maria M. Picken MD, PhD mpicken@lumc.edu
Nephron = functional & structural unit - glomerulus - proximal tubule - loop of Henle, - distal tubule collecting duct system - kidneys produce 125 ml of filtrate/minute - 124 ml is reabsorbed - approximately 1.5 L of urine/day nephros – greek = kidney
Two general classes of nephrons: cortical (superficial, 6/7) and juxtamedullary nephrons (1/7): important in producing hypertonicity in medullary interstitium – see physiology lecture. Both types are classified according to the length of their associated loop of Henle and location of their glomerulus. While all nephrons have their glomeruli in the cortex, cortical nephrons have their loop of Henle in the renal medulla near its junction with the renal cortex, while the loop of Henle of juxtamedullary nephrons is located deep in the renal medulla; they are called juxtamedullary because their glomerulus is located near the medulla (but still in the cortex).
* ^^ • Proximal convoluted tubule (PCT) - high cuboidal to low columnar epithelium: • prominent brush border (*) to increase reabsorption, (carbonic anhydrase on apical surface, • 80-90% of bicarbonate reabsorbed) • many mitochondria • basal infoldings (^^) abutting on fenestrated capillaries with diaphragms
NEPHRON – SUMMARY – see physiology and pharmacology lectures Proximal convoluted tubule: - reabsorption of 2/3 of water • 100% of proteins <70,000 MW • 2/3 of Na+ primarily with Cl- (transcellular and paracellular pathways) • all glucose, amino acids • 80-90% bicarbonate • production of Calcitriol (control of Ca2+ homeostasis) Loop of Henle: descending and ascending limb (hairpin), thin and thick portions with the vasa recta form the counter current exchanger - urinary concentration descending limb is freely permeable to water while ascending limb is impermeable (ascending limb considered by some to be part of the distal tubule) • 25% of Na+reabsorbed here • maximal osmolarity at tip 4x blood Distal convoluted tubule: numerous mitochondria (ATP for active transport), macula densa • all remaining Na+Cl- and water • excretion of K+ • secretion ofH+and ammonium to regulate pH • aldosterone (adrenal cortex)stimulates Na+ & water reabsorption and excretion of K+ & H+ in urine = control of total salt and water in urine - parathyroid hormone – increased reabsorption of calcium and secretion of phosphate - atrial natriuretic peptide: increase sodium secretion. Collecting duct - receptors for antidiuretic hormone (posterior pituitary),increases permeability to water, which goes into interstitium. If no antidiuretic hormone, watery urine. Beer and caffeine antidiuretic hormone. - permeability to urea
Pathology – “medical”: • glomerular versus tubular • renal failure • HTN (hypertension) • anemia, hyperparathyroidism Because of its importance in body fluid regulation, the nephron is a common target of drugs that treat high blood pressure and edema. These drugs, called diuretics,inhibit the ability of the nephron to retain water, thereby increasing the amount of urine produced Pathology – “surgical” • tumors: nephron, in particular proximal tubule • NOT glomerulus
Renin granules Electron microscopy Vascular pole visceral epithelial cells (podocytes) aka extraglomerular mesangial cells Juxtaglomerular apparatus: - at the vascular pole of the glomerulus • afferent + efferent arterioles + macula densa + extraglomerular mesangial cells regulates glomerular filtration rate depending on tubular luminal concentration of Na+/Cl- “tubuloglomerular feedback”
Juxtaglomerular apparatus: macula densa of distal convoluted tubule +afferent + efferent arterioles + extraglomerular mesangial cells - macula densa: cells taller (columnar) with more prominent nuclei, thin basement membrane → can communicate with the cells of the underlying arteriole • juxtaglomerular cells (aka “granular cells”): mainly in the wall of afferent arteriole, modified smooth muscle cells, production and secretion of the enzyme renin (stored in the granules) - decreased loads of NaCl in distal nephron promotes renin release whileincreased NaCl inhibits - renin is also released in response to renal sympathetic activity and - decreased intrarenal blood pressure (<90mmHg systolic blood pressure) Renin increases blood pressure indirectly as it activates the angiotensin system
Renin increases blood pressure indirectly as it activates the angiotensin system Angiotensin precursor, angiotensinogen, is produced constitutively and released into the circulation mainly by the liver. Angiotensin I is formed by the action of renin on angiotensinogen. Angiotensin I is converted to angiotensin II by the enzyme angiotensin-converting enzyme (ACE). Angiotensin (a hormone) causes vasoconstriction and a subsequent increase in blood pressure. Angiotensin also stimulates the release of aldosterone (hormone) from the adrenal cortex, which promotes sodium retention in the distal nephron. This also drives up blood pressure. Renin-angiotensin system is a major target for drugs that lower blood pressure
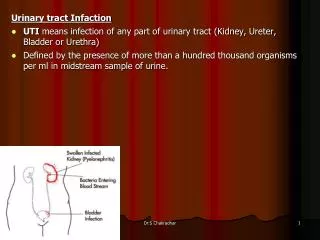
The normal ureter is a conduit to drain urine effectively at low pressures from the kidney to the bladder.
transitional epithelium (urothelium) lamina propria with discontinous muscularis mucosae muscularis (detrusor muscle, aka deep muscle)
The urothelium (aka transitional epithelium) lines the renal pelvis, the ureters, the bladder, and parts of the urethra. Urothelium consists of approximately 3-5 cell layers, which can contract and expand. The term transitional epithelium does not imply that this epithelium is in actual transition from one type to another, but rather refers to the appearance of the cells, which change as the organs with which they are associated are stretched or relaxed. These cells appear to be cuboidal when the organ or the tube in which they reside is not stretched. When the bladder fills, the cells become stretched, and they appear to be flat. http://www.meddean.luc.edu/lumen/MedEd/urology/abnurtdv.htm non-distended (relaxed) bladder distended bladder
The transitional epithelium cells • accommodate the fluctuation in volume of the contained liquid • protect against the caustic effects of urine - a powerful barrier to urine • The superficial bladder epithelium (umbrella cells): • apical exocytosis of specialized fusiform vesicles (aka discoid vesicles) during distension of the bladder provides additional fragments of cell membrane, which can incorporate into the cell membranes, allowing them to stretch in a full bladder. • 2. the apical plasma membrane of umbrella cells, facing the urine, is covered with rigid-looking plaques, which, together with tight junctions, form a specialized membrane compartment that represents one of the tightest and most impermeable barriers in the body. • Transitional carcinoma: bladder, pelvis, ureter, urethra
Female versus male urethra – connected with the reproductive system
Questions? mpicken@lumc.edu