Download
1 / 9
90 likes | 178 Vues
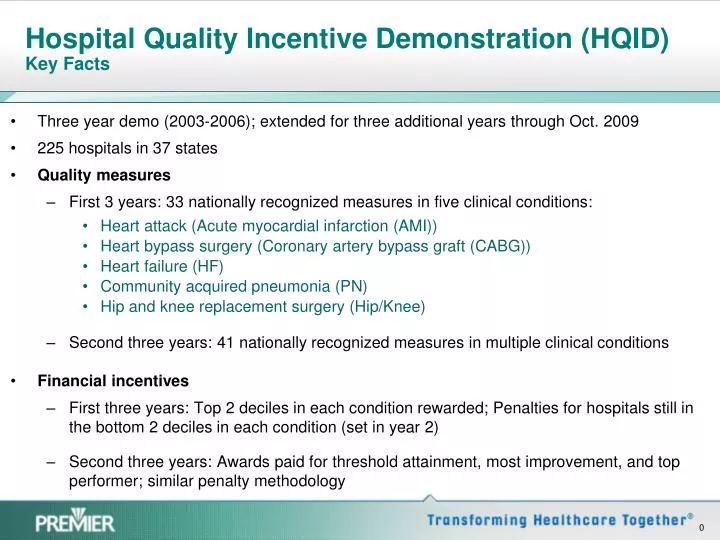
Hospital Quality Incentive Demonstration (HQID) Key Facts. Three year demo (2003-2006); extended for three additional years through Oct. 2009 225 hospitals in 37 states Quality measures First 3 years: 33 nationally recognized measures in five clinical conditions:

E N D
Hospital Quality Incentive Demonstration (HQID)Key Facts • Three year demo (2003-2006); extended for three additional years through Oct. 2009 • 225 hospitals in 37 states • Quality measures • First 3 years: 33 nationally recognized measures in five clinical conditions: • Heart attack (Acute myocardial infarction (AMI)) • Heart bypass surgery (Coronary artery bypass graft (CABG)) • Heart failure (HF) • Community acquired pneumonia (PN) • Hip and knee replacement surgery (Hip/Knee) • Second three years: 41 nationally recognized measures in multiple clinical conditions • Financial incentives • First three years: Top 2 deciles in each condition rewarded; Penalties for hospitals still in the bottom 2 deciles in each condition (set in year 2) • Second three years: Awards paid for threshold attainment, most improvement, and top performer; similar penalty methodology
Dramatic and Sustained Improvement CMS Value-based Purchasing Demonstration Composite Quality Score Avg. improvement across all 5 clinical areas for median CQS (24 quarters) 18.8%
More Patients are Reliably Receiving Evidenced-based Care Evidence-based Care Improvements Avg. improvement from 4Q03 to 3Q09 in all clinical areas (24 quarters) 55.7% Appropriate Care Score
Improvement Across All VBP demo Participants Pneumonia CMS Quality Score Threshold Changes by Year • Quality improvement across all hospitals • Variation in hospital performance decreased Heart Failure CMS HQID Quality Score Threshold Changes by Year CABG CMS Quality Score Threshold Changes by Year
Improvement and Savings Over Three Years Avg. improvement in mortality across four clinical areas 1.87% Avg. cost improvement per patient across all clinical areas $1,063 If all hospitals in the nation were to achieve this improvement, the estimated cost savings would be greater than $4.5 billionannually with estimated 70,000 lives saved per year
Relationship between hospital type and performance • No relationship between hospital performance and urban/rural or bed size status • Relationship between safety-net status and performance: • Safety net hospitals (11.75% DSH) initially started out with lower quality scores as a group. • While safety-net hospitals improved performance, as a group, they tended to cluster below the median. • However, safety-net hospital were equally represented in the top 20% by the third year. • Therefore, we found no statistically significant disparity for top performance in the third year for safety-net hospitals.
Acute myocardial infarction (AMI) Aspirin at arrival Aspirin prescribed at discharge ACEI/ARB for LVSD Smoking cessation advice/counseling Beta blocker prescribed at discharge Beta blocker at arrival Thrombolytic received within 30 minutes of hospital arrival PCI received within 90 minutes of hospital arrival Inpatient mortality rate Coronary artery bypass graft (CABG) Aspirin prescribed at discharge CABG using internal mammary artery (Test) Prophylactic antibiotic received within one hour prior to surgical incision Prophylactic antibiotic selection for surgical patients Prophylactic antibiotics discontinued within 24/48 hours after surgery end Patients with controlled 6 A.M. Postoperative Blood Glucose Inpatient mortality rate Post operative hemorrhage or hematoma Post operative physiologic and metabolic derangement Hip and knee replacement Prophylactic antibiotic received within one hour prior to surgical incision Prophylactic antibiotic selection for surgical patients Prophylactic antibiotics discontinued within 24 hours after surgery end time Post operative hemorrhage or hematoma Post operative physiologic and metabolic derangement Readmission within 30 days to any acute care facility Surgery patients with recommended VTE prophylaxis ordered Surgery patients who received appropriate VTE prophylaxis within 24 hours prior to surgery up to 24 hours after surgery end time Heart failure (HF) Left Ventricular Systolic (LVS) assessment Detailed discharge instructions ACEI or ARB for LVSD Smoking cessation advice/counseling Pneumonia (PN) Percentage of patients who received an oxygenation assessment within 24 hours prior to or after hospital arrival Initial antibiotic selection for Community Acquired Pneumonia Blood culture collected prior to first antibiotic administration Influenza screening/vaccination Pneumococcal screening/vaccination Antibiotic timing, percentage of pneumonia patients who received first dose of antibiotics within four/six hours after hospital arrival Smoking cessation advice/counseling Surgical Care Improvement Project (SCIP) (year 5 & 6) Prophylactic antibiotic received within 1 hour prior to surgical incision Prophylactic antibiotic selection for surgical patients Prophylactic antibiotics discontinued within 24 hours after surgery end Patients with controlled 6 A.M. Postoperative Blood Glucose Surgical Patients with Hair Removal Colorectal Surgery Patients with Normothermia Surgery patients with recommended VTE prophylaxis ordered Surgery patients who received appropriate VTE prophylaxis within 24 hours prior to surgery up to 24 hours after surgery end time Surgery patients on Beta-Blocker Therapy who Receive Beta-Blocker during Perioperative Period Widely Accepted Clinical Indicators Used in CMS VBP demonstration(Measures added for Years 4&5 = Red text)Outcomes measures (7) = Bold italicized textComposite score an average of all measures for each condition
In Broader Comparison, Hospitals in VBP Demonstration Excel National Leaders in Quality Performance HQID hospitals have higher quality ratings* than national hospitals overall *CMS process score • VBP demonstration participants avg. 6.5% higher than Non-Participants in first 3 ½ years of demo • Avg. improvement for HQID participants = 7.8% • Avg. improvement for Non-participants = 5.6% • New England Journal of Medicine publication by Lindenauer et al. (February 2007) found that hospitals engaged in P4P achieved quality scores 2.6 to 4.1 percentage points above other hospitals due solely to the impact of P4P incentives. A composite of 19 measures shared in common between HQID and Hospital Compare shows P4P hospitals performing above the nation as a whole
Example: Reliable Care Improves Readmissions, Mortality, Cost and Length of Stay Outcomes Data indicate fewer complications are associated with better care Data show lower mortality rates for heart bypass surgery patients receiving better care Heart bypass surgery patients with complications(%) Mortality rate of heart bypass surgery patients (%) Complications Mortality Rate Patient Process Measure Patient Process Measure Data indicate fewer readmissions are associated with better care Data show fewer hospital days associated with patients receiving better care Mortality rate of heart bypass surgery patients (%) Average LOS for heart bypass surgery patients Patient Readmissions (%) Average LOS (days) Patient Process Measure Patient Process Measure