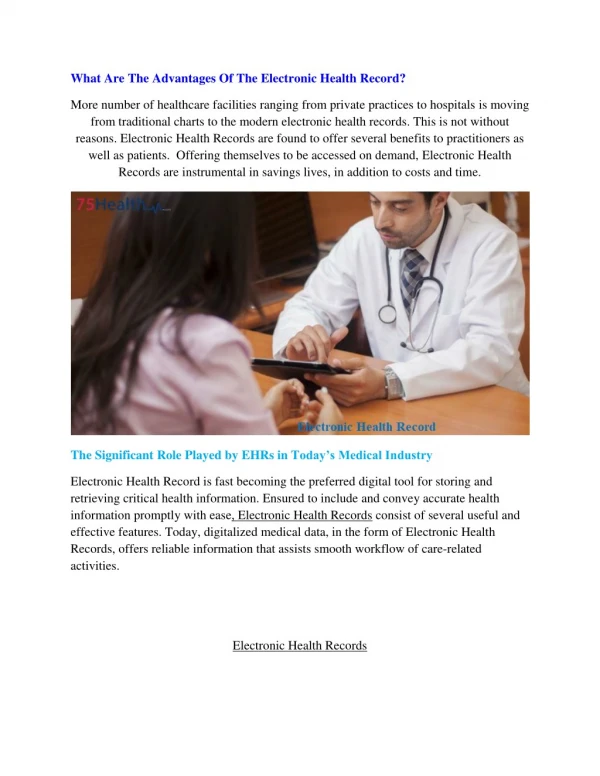
Download
1 / 22
230 likes | 379 Vues
Coordination of Terminologies and Classifications in Electronic Health Records. Sue Bowman, RHIA, CCS Director, Coding Policy and Compliance American Health Information Management Association. EHR Interoperability. Interoperable health information exchange requires common medical language

E N D
Coordination of Terminologies and Classifications in Electronic Health Records Sue Bowman, RHIA, CCS Director, Coding Policy and Compliance American Health Information Management Association
EHR Interoperability • Interoperable health information exchange requires common medical language • Common medical language is represented by linked, standard terminologies and classifications
Organizational Decisionmaking Today’s Reality Patient Reimbursement Severity Measurement Medical Record Coding Disease Management & Registries Database Operational Decision making Statistics
Organizational Decisionmaking Ideal Process Patient Reimbursement Coding Severity Measurement Medical Record SNOMED CT Disease Management & Registries Database Operational Decision making Statistics
Terminologies & Classifications – Why Both? • Different roles and purposes • Terminology – “input” system • set of terms describing health concepts • “reference terminology” is an explicit, formal specification or ontology of concepts and the relationships linking them • Used to record detailed clinical information to support clinical care, decision support, outcomes research, and quality improvement • Classification – “output” system • Groups together similar diseases and procedures and organizes related entities for easy retrieval • Used for external reporting purposes, such as reimbursement and statistical and epidemiological data analysis
Terminology (SNOMED) APGAR: cardiac score, respiratory score, muscle tone, reflex response, color, etc. Classification (ICD-9-CM) Final diagnosis : normal newborn Procedure: Circumcision Classifications and Terminologies Capture Different Levels of Clinical Detail
Reference Terminologies • Reference Terminologies • SNOMED-CT • LOINC • NDF-RT • RxNorm
Classification Systems • Classifications • ICD-9-CM • ICD-10-CM • ICD-10-PCS • ICD-O • ICF • ICPC • HCPCS
Role of Mapping • “Mapping” is the process of linking content from one terminology to another or to a classification • Reference terminologies mapped to modern classification systems • Decrease administrative costs • Decrease time in revenue cycle • Increase specificity and accuracy of data • Maintain comparable data
Map Development • Define use case (intended purpose) • Unidirectional vs. bidirectional • Testing and validation • Ongoing maintenance and updating
Use Case Specification • Intended users must be clearly defined • Context of the use case is important • Multiple use cases are possible between the same 2 terminologies • Stating the map’s purpose is first step to defining scope, level of validation, and intended audience • Use case becomes framework for additional requirements for the map
Mapping Principles • Understandable • All mappings have stated purpose and audience • Map documentation is complete, clear, and unambiguous • Mappings define source & target domain scope for the map
Mapping Principles (con’t) • Reproducible • Mappings employ authoritative reference sources uniformly • Documentation defines all assumptions, heuristics, and procedures required to manage context and create map • All terminology developers move to compliance with sound principles of permanence and version management
Mapping Principles (con’t) • Useful • Use cases are defined for map • Publication cycle is timely and linked to version change for source & target vocabularies • Agreement is reached for standards of knowledge representation in mapping
Examples of Maps • ICD-9-CM 2005 to ICD-9-CM 2006 • ICD-9-CM Vol III to CPT (and vice versa) • DSM-IV to ICD-9-CM • SNOMED CT to ICD-9-CM • SNOMED CT to nursing terminologies • SNOMED CT to LOINC
Mapping Issues • Different maps are needed for different use cases • There are no map development standards • Validation of map is critical • Mapping process is dynamic • Definition of “valid” map is needed • Managing context (patient characteristics, comorbid conditions, encounter data, etc.) is challenging • Complexity of coding rules for administrative reporting also creates challenges • Human review has not been eliminated • Map development is still in its infancy
Other Harmonization Issues • Code set development/maintenance disparities • Need better coordination among code set developers and maintenance organizations to facilitate development of better maps • Harmonization of code set effective dates would facilitate map maintenance process • Continued use of outdated classification systems • Replacement of ICD-9-CM with ICD-10-CM/PCS would result in improved maps from terminologies
Resources • AHIMA web site • www.ahima.org • AHIMA’s white paper titled “Coordination of SNOMED-CT® and ICD-10: Getting the Most Out of Electronic Health Record Systems” • http://library.ahima.org/xpedio/groups/public/documents/ahima/bok1_027179.html