Download
1 / 32
370 likes | 1.24k Vues
Explore the latest advances and challenges in treating cancer pain, including breakthrough pain and opioid therapy. Learn about opioid rotation and managing adverse effects for optimal pain relief.

E N D
New Treatment Paradigm in Cancer Pain Management Nicole NACCACHE, M.D. Service d’AnesthésieRéanimation et de Douleur HôtelDieu de France
Prevalence of Cancer and PAIN (WHO) 18.1 millioncases (14 million 2012) 9.6 million cancer death Estimated cancer In 2018 21.7 million new cases 13 million deaths Estimated cancer in 2030 50% report SEVERE PAIN 80% advanced cancer with moderate to severe pain Cancer pain International Agency for Research on Cancer (WHO)- Sept 2018- Press Release N=263
Cancer Pain Unmet Clinical Need • EFIC survey evaluated pain in 4947 people with cancer • Pain prevalence is 72% • 23% did not receive pain medication • EFIC in depth analysis in 573 people • Incidence of breakthrough pain 63% • Experience persistent pain in 58% Cancer pain is poorly recognized and treated Breivik H et al. Ann Oncol 2009; [online Feb 24, 2009; doi:10.1093/annonc/mdp001].
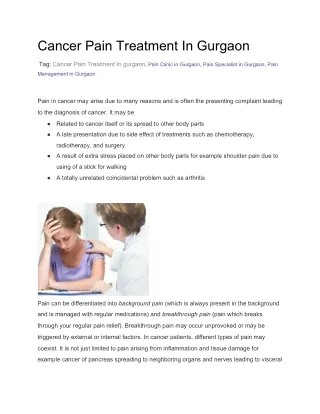
Cancer Pain Chronic cancer pain is composed of two parts: • Persistent pain • Breakthrough pain (BTcP) • Persistent pain: Baseline • Constant or continuous pain that is experienced by the patient for more than 12 hours per day • Portenoy RK and Hagen NA. Prim Care Cancer1991:27–33.
“A transient exacerbation of pain that occurs despite relatively stable and adequately controlled background pain” Cancer: What is Breakthrough Pain? Adapted from Bennett D et al,1 and Portenoy and Hagen2 BTcP refers to the pain flares that occur beyond the baseline persistent pain
Bennett D et al. Part I. P&T 2005;30:296–301. Breakthrough Pain: Clinical Features BTcPis characterised by rapid onset, short duration and severe intensity
Breakthrough Pain: ImplicationsPhysical / Psychological / Social(Zeppetella, ClinOncol 2011; 23: 393–398)
Pain: Persistent v/s Breakthrough (Portenoy 1999 / Davis 2009)(EONS Breakthrough Pain Guidelines 2013)
Cancer Pain and its Challenges Management of cancer pain • Opioids: mainstay of cancer pain therapy • “TheRight dose” the one that relieve pain No standard dose - WHO guidelines: appropriate use
Baseline Pain Management WHO 3 steps ladder v/s NCCN Guidelines WHO1 NCCN2 World Health Organization. Cancer pain relief: with a guide to opioid availability. 2nd ed. Geneva:The Organization;1996. National Comprehensive Cancer Network (NCCN) GuidelinesTM Ver. 2.2011: Adult Cancer Pain
Principle for safe & effective opioid useGreat variation in opioid dose The correct dose is the dose that works (WHO) Adverse Events Pain free – trust the patient Dose of Opioid PainIntensity Titrate to effect = dose finding Time
Administration of analgesic therapies According to the World Health Organization (WHO), Analgesics should be administered
Uncontrolled PainBaseline v/s Breakthrough Clinical features BTcP must be distinguished from uncontrolled background pain
Breakthrough painOpioid rescue medication(EONS, Breakthrough Pain Guidelines 2013)
Failed opioid treatment: When? • Insufficient analgesia after 2–3 dose increases and/or • Unacceptable adverse effects (Myoclonus /Delirium /Insomnia /NV/Resp. dep /Sedation) Opioid rotation Another opioid to be considered Switching one level III WHO opioid • Improving pain relief • Reducing intensity of adverse effects Mercadante S. Cancer 1999,86;9:1856
Tolerance Opioid Induced Hyperalgesia (OIH) Tolerance - Loss of drug potency - Desensitization of nociceptive pathways to opioids • Increase in opioid dose result in reduction of pain OIH - Caused by exposure to opioids - Increased pain sensitivity and involves pro-nociceptive pathways - OIH will worsen with an increase in opioid dosage
Need for Opioid rotation: Why? • Why to switch? • Inter-individual variability in patient response to different opioids • Opioid receptor mutation • Altered binding affinities • - Conformational changes of opioid receptor Vadalouca A, et al. J Opioid Manag 2008;4:213
Need for Opioid rotation: When? • 1/3 patients treated with opioids needs rotation (Fine PG, JPSM 2009) • When to switch? • Inadequate analgesia • Dose-limiting adverse effects Vadalouca A, et al. J Opioid Manag 2008;4:213
Rotation RecommandationsEAPC – AWNF – NHS – NCCN EAPC: European Association of Palliative Care (2012) AWMF: Guidelines for Palliative Med (2015) • Morphine,Oxycodone,Hydromorphoneareequivalent first-line opioids • Second-line opioid: dose reduction followed by retitration NHS: National Health Service (2014) • Rotation: in case of intolerable side effects with or without good analgesia • Second-line opioid: doses reduced by 30% and retitrated NCCN: National Comprehensive Cancer Network (2016) - Rotationif Pain score more 4 ;Nausea for 1 week ;Sedation more than 2-3 days Constipation consider Fentanyl patch
EquianalgesicconversionInternational guidelines . National Opioid Use Guideline Group, 2010
Guidelines for opioids rotation Ashburn MA, Glenview (IL): American Pain Society; 2003.
New TreatmentParadigm OXYCODONE
Oxycodone hydrochloride: Formulations • Oxycodone used clinically for more than 80 years (1916 Germany) • Oxycodone = Immediate release (IR) oral capsules(5, 10 and 20mg)(BREAKTHROUGH) • Oxycontin= Prolonged release (PR) tablets (5, 10, 20, 40 and 80mg) (Opioid Rotation) • Oxynorm = Oxycodone injection 10 mg/ mL (ampoule 1 ou 2ml) 1 mg of IV oxycodone = 1 mg of IV morp .
Characteristics of oxycodone Analgesic potency twice that of morphine Some κ-agonist activity Effective in a broad range of moderate-to-severe chronic pain >60% oral bioavailability No ceiling dose Metabolized by CYP3A4 / CYP2D6 Negligible clinical impact of metabolites Riley J et al. Curr Med Res Opin2008;24(1):175-192; Levy MH et al.Eur J Pain 2001;5(Suppl. A):113-116- Biancofiore G. TherClin Risk Manage 2006;2(3):229-234.
Oxycodone SR Innovative delivery system • Biphasic release and absorption • Rapid release: early onset of analgesia • Sustained second phase:effectiveblood concentrations for 12h Curtis GB et al. Eur J ClinPharmacol1999;55(6):425-429; Sunshine A et al. J ClinPharmacol 1996;36(7):595-603; -. Citron ML et al. Cancer Invest 1998;16(8):562-571.
Oxycodone Analgesic efficacy in moderate/severe pain • Cancer pain • Neuropathic pain • Somatic pain • Visceral pain • Acute postoperative pain
Oxycodone SR Effective in Severe Cancer Pain • Mean Final daily doses: 100mg Oxy v/s 140mg Morp • Oxycodone SRand morphine SR are similarly effective in cancer pain Patients achieving stable pain (%) Patients rating therapy as good or excellent (%) Mucci-LoRusso P, et al. Eur J Pain 1998;2(3):239-249.
Oxycodone SR Effective in Cancer Pain Rapid onset of analgesic action occurred within 1h in 198 cases (91.7%) of patients following administration of oxycodone SR % of patients Time of onset Pan H et al. Clin Drug Invest 2007;27(4):259-267.
Chronic visceral pain Therapeutic approaches • Modulation of peripheral sensory processing • K-opioid agonists • Modulation of central sensory processing • Opioid-induced hyperalgesia 1. Staahl C et al. Basic Clin. PharmacolToxicol 2006;98(2):201-211.
Oxycodone: Ease of Titration • Dose titration is achieved quickly (plasma levels reached within 24 hours) • Choice of formulations increases flexibility • Wide choice of doses increases compliance • Immediate release is available for breakthrough pain in cancer pain management • Adverse event (AE) similar to other strong opioids • Oxycodone SR must never be crushed, chewed or broken can lead to overdose 1. Benziger D et al. Pharmacotherapy 1995;15(8):391.
Conclusions Persistent v/s Breakthrough Pain Different entity Opioid rotation is to be considered in dose limiting effect or side effects Oxycodone is effective as a first line or as an alternative treatment to morphine .