Download
1 / 22
220 likes | 376 Vues
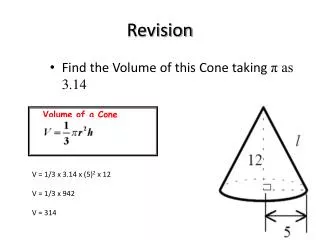
Advanced Medical Science. REVISION. What is mitral insufficiency? Define the term heart failure, and outline right and left heart failure. What is the difference between hypovolemic shock and cardiogenic shock? Using a diagram, explain what happens during hypovolemic shock.

E N D
Advanced Medical Science REVISION What is mitral insufficiency? Define the term heart failure, and outline right and left heart failure. What is the difference between hypovolemic shock and cardiogenic shock? Using a diagram, explain what happens during hypovolemic shock. ITP occurs when circulating immunoglobulin ___ molecules react with host _____________. Iron ___________ ___________ is a disorder of ___________ transport in which the ___________ of _______________ is inadequate. Iron deficiency anaemia can result from ______________ , __________________ and _________________.
REVISION Which of the following is the normal life span of an RBC? 90 days 120 days 100 days 2 days Thrombocytopenia is characterised by: Not enough circulating platelets Too many circulating platelets Decreased RBC production Increased RBC production 3. Extrinsic Asthma is caused by: Sensitivity to specific allergens Severe respiratory tract infection Emotional stress Exogenous dissemination
REVISION Outline the pathophysiology of dilated cardiomyopathy. Regarding Tension Pneumothorax, what is impaired during inspiration ? Identify and explain the 3 ways in which pneumonia is classified. Also called __________ ________, Down Syndrome is caused by an aberration in which ____________ _________ has three copies instead of _________. Respiratory syncytial virus occurs almost exclusively in __________ and ___________ ___________. Tay-Sachs disease results from a _______________ _____________ _______________. MI results from ________________ blood flow through one of the _______________ arteries. This causes myocardial ______________ , injury and necrosis.
REVISION Identify two areas of the body that can indicate cyanosis. Acute respiratory distress is a form of pulmonary _____________. Explain the pathophysiology of ARDS. Outline 3 pathophysiologic changes during an asthma attack. What type of cell is transformed within a patients airway, in lung cancer? In bacterial pneumonia, an ________________ triggers alveolar ________________ and _____________. This produces an area of low _________________ with ______________ perfusion. In viral pneumonia, the ___________ attacks _____________ epithelial ____________, causing ______________ _________ and desquamation. The ____________ also invades ____________ glands and goblet ____________ spreading to the ______________, which fill with blood and fluid.
Disorders of Renal Function Diseases of the kidney and urologic tract can strike anyone at any age. Some of these disease are progressive, eventually leading to chronic kidney disease and the need for dialysis and transplantation. The kidneys filter blood from all parts of the body, and although, many forms of kidney disease originate in the kidneys, others develop secondary to disorders such as hypertension, type II diabetes and SLE.
Glomerulonephritis Bilateral inflammation of the glomeruli, commonly following a streptococcal infection. Acute glomerulonephritis is most common in boys ages 3 to 7, but it can occur at any age. Rapidly progressive glomerulonephritis most commonly occurs between ages 50 and 60. It may be idiopathic or associated with a proliferative glomerular disease such as post-streptococcal glomerulonephritis. Chronic glomerulonephritis is a slowly progressive disease characterised by inflammation, sclerosis, scarring and eventual renal failure. It usually remains undetected until the progressive phase, which is irreversible. Pathophysiology: In nearly all types of glomerulonephritis, the epithelial layer of the glomerular membrane is disturbed. Acute post-streptococcal glomerulonephritis results from entrapment and collection of antigen-antibody complexes in glomerular capillary membranes after infection with a group A beta-haemolytic streptococci. The antigens stimulate the formation of antibodies. Circulating antigen-antibody complexes become lodged in the glomerular capillaries.
Glomerulonephritis Glomerular injury occurs when complexes initiate the release of immunologic substances that break down cells and increase membrane permeability. The severity of glomerular damage and renal insufficiency is related to size, number, location, duration of exposure, and type antigen-antibody complexes. Signs and symptoms: decreased urination or oliguria, coffee-coloured urine, shortness of breath, orthopnoea, mild to severe hypertension, nausea, malaise and arthralgia. Blood Testing: BUN and Creatinine are elevated; Serum protein levels are decreased; Hb levels may decrease in chronic glomerulonephritis.
Glomerulonephritis Good pasture Syndrome is an uncommon and aggressive form of glomerulonephritis. In Good pasture’s syndrome, antibodies are produced against the pulmonary capillaries and glomerular basement membrane. Glomerular filtration rate becomes reduced, and renal failure occurs within weeks or months. Pathophysiology: The cause of the disorder is unknown, although influenza infection and exposure to hydrocarbon solvent have been implicated in some individuals, as have various drugs and cancers.
Glomerulonephritis Pathophysiologic Changes Decreased glomerular filtration rate (GFR): Decreased urination or oliguria. Haematuria: Smoky or coffee-coloured urine. Hypervolemia: Dyspnoea and orthopnoea; oedema Decreased GFR, sodium or water retention, and inappropriate release renin: Mild to severe hypertension.
Glomerulonephritis: How It Happens Robinson, J.M. 2005. Pathophysiology: Just the Facts.
Pyelonephritis Pyelonephritis refers to infection of the kidney parenchyma and renal pelvis. There are two forms of pyleonephritis, acute and chronic. Chronic pyelonephritis is a more complex disorder involving not only bacterial infection but also other factors such as reflux. Acute Pyelonephritis: represents a bacterial infection of the upper urinary tract, specifically the kidney parenchyma and the renal pelvis. Gram negative bacteria , including E.Coli and Proteus, Klebsiella , Enterobacter, and pseudomonas species, are the most common causative agents. The onset of acute pyelonephritis is usually abrupt, with shaking chills, moderate to high fever and a constant ache in the loin area of the back that is unilateral or bilateral. Lower urinary tract symptoms, including dysuria, frequency, and urgency are also common. There may also be significant malaise.
Pyleonephritis Chronic pyelonephritis: represents a progressive process. There is scarring and deformation of the renal calyces and pelvis, along with atrophy and thinning of the overlying cortex. Pathophysiology: The disorder involves a recurrent or persistent bacterial infection superimposed on urinary tract obstruction, urine reflux, or both. Chronic obstructive pyelonephritis can be bilateral, caused by conditions that obstruct bladder flow, or unilateral, such as occurs with ureteral obstruction. Reflux, which is the most common cause of chronic pyleonephritis, results from superimposition of infection on congenital vesicoureteral reflux or intrarenal reflux.
Vesicoureteral Reflux Porth, C.M. 2011. Essentials of Pathophysiology, 3rd edn.
Chronic Pyelonephritis Porth, C.M. 2011. Essentials of Pathophysiology, 3rd edn.
Drug-Related Nephropathies Drug-related nephropathies involve functional or structural changes in the kidneys that occur after exposure to a drug. Because of their large blood flow and high filtration pressure, the kidneys are exposed to any substance that is in the blood. Drugs and toxic substances can damage the kidneys by causing a decrease in renal blood flow urine flow, directly damaging tublointerstital structures, or producing hypersensitivity reactions.
Obstruction Causes urine to accumulate behind blockage in urinary tract leading to infection or damage. May be congenital or acquired, acute or chronic Acute, complete obstruction increases pressure transmitted to proximal tubule, inhibiting glomerular filtration. Chronic, partial obstruction compresses structures as urine accumulates; results in papillary and medullary infarct; underlying tubular damage decreases kidneys ability to function. Tubular obstruction increases interstitial fluid pressure; if unrelieved, causes nephron and capillary collapse and irreversible renal damage. Relief is usually followed by copious diuresis of sodium and water and return to normal GFR.
Renal Calculi Renal calculi, or kidney stones, may form anywhere in the urinary tract, but they usually develop in the renal pelvis or calices. Calculi form when substances that normally dissolve in the urine precipitate. They vary in size, shape and number. Pathophysiology: Although their exact cause is unknown, there are several predisposing factors: Dehydration: decreased water and urine excretion concentrates calculus forming substances. Infection: infected, scarred tissue provides a site for calculus development. Calculi may become infected if bacteria are the nucleus in calculi formation. Changes in Urine pH: Consistently acidic or alkaline urine provides a favourable medium for calculus formation. Obstruction: urinary stasis allows calculus constituents to collect and adhere, forming calculi. Obstruction also encourages infection, which compounds infection.
Renal Calculi Pathophysiology: Immobilisation: immobility from spinal cord injury or other disorders allows calcium to be released into the circulation and eventually, to be filtered to the kidneys. Diet: Increased intake of calcium or oxalate-rich foods encourages calculi formation. Metabolic factors: hyperparathyroidism, renal tubular acidosis, elevated uric acid (usually with gout), defective oxalate metabolism, a genetic defect in cystine metabolism, and excessive intake of Vitamin D or dietary calcium may predispose a person to renal calculi. Types of Stones: There are four types of kidney stones; oxalate or phosphate, magnesium ammonium phosphate stones, uric acid stones and cystine stones.
Renal Calculi: How it Happens Urine becomes concentrated with insoluble materials Crystals form Mucoprotein is reabsorbed Calculi remain in the renal pelvis and damage or destroy kidney tissue Pressure Necrosis Calculi obstruct urine Hydrostatic pressure increases Irreversible damage
Hydronephrosis An abnormal dilation of the renal pelvis and the calyces of one or both kidneys, hydronephrosis is caused by an obstruction of urine flow in the genitourinary tract. Pathophysiology: Almost any type of disease that results from obstruction of the urinary tract can result in hydronephritis. The most common causes are: Benign prostatic hyperplasia Urethral strictures Stenosis of the ureter or bladder outlet Congenital abnormalities Abdominal tumours Blood clots Neutrogenic bladder Tumours of the ureter and bladder.