ULCERATIVE COLITIS A CASE DISCUSSION
ULCERATIVE COLITIS A CASE DISCUSSION. By Dr.Syed Hunain Riaz PG-1 M-2. CASE HISTORY.

ULCERATIVE COLITIS A CASE DISCUSSION
E N D
Presentation Transcript
ULCERATIVE COLITISA CASE DISCUSSION By Dr.Syed Hunain Riaz PG-1 M-2
CASE HISTORY A 25 year old male presented with 7 months on and off history of blood in stools with a frequency of around 7-8 loose stools per day. The onset of bloody stools was insidious in nature. The stools were small in amount, watery in consistency, and mixed with blood, which was fresh in color, there is no history of mucus or pus in stools.There stools were not foul smelling. There was associated history of abdominal pain which was crampy in nature and was localized to central abdomen and sometimes the left loin and often relieved by passing stools. There was history of incomplete evacuation. There was no history of peri-anal pain during defecation and no previous history of long standing constipation. There was no history vomiting. There is history of on and off fever over the last 6-7 months which varied between low and high grade and he did not take any medication for it, and it was relieved by itself. There is no history of joint pains, yellowness of eyes, back pain or pruritis. The patient does appreciate weight loss over the last many months. There is no history of abdominal distention or body swelling.
Family history reveals no significant information. • Patient is a non-smoker and non-addict. • There is no history of i/v drug abuse or any blood transfusions in the past. • On inquiry there appears to be no history of any personal loss or any social trauma. • He is non-diabetic.
Examination • An thin lean young male lying lazily in bed well oriented in time place and person. GENERAL PHYSICAL EXAM: No pallor, jaundice, clubbing, lymph nodes, skin lesions, mouth ulcers, there appear to be signs of dehydration. BP: 110/70 mm Hg Pulse: 100/min R/R: 16/min There is no swelling in front of neck. GASTROINTESTINAL EXAM: Abdominal flat and soft with an inverted umbilicus, no obvious swelling or deformity. No visceromegaly detected, no mass palpable.Slight tenderness in the left flank. Bowel sounds audible and 10-15 in frequency. Peri anal exam reveals no anal tags, no abcess EXAMINATION OF OTHER SYSTEMS DID NOT REVEAL ANY FINDINGS
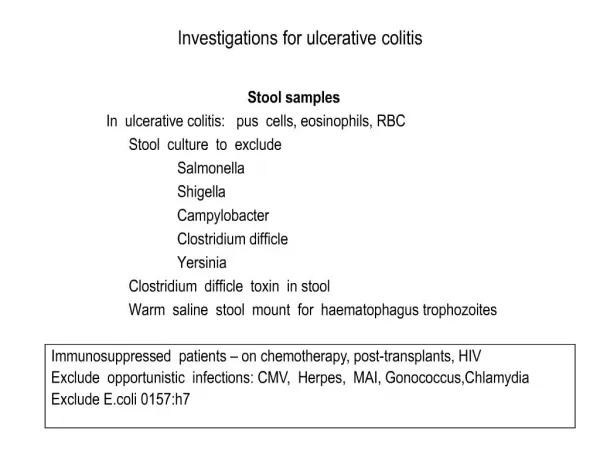
Investigations • Stool Examination 1.Revealed no ova or parasites 2. Leucocytes were detected and 3. Obviously stool was positive for blood. • Complete blood count: Hb: 11g/dl TLC: 7000/mm³ Platelets: 255,000/mm³ • ESR: 15 mm/1st hour
CRP: Normal • LFT’s: ALT, AST and bilirubin within limits • S\Albumin: 3.7 g/dl • USG Abdomen: Scan was normal, especially liver and biliary tract. • Chest Xray: Revealed no findings.
Urine Complete exam: Did not reveal any pus cells, rbc’s or calcium oxalate crystals. Now based on history and basic clinical examination and routine investigations, our list of differentials will include:
Differential diagnosis • Ulcerative colitis • Infective colitis • Crohn’s colitis • Irritable bowel syndrome • Malignancy of the gut i.e CA colon, lymphoma
Now to further differentiate between infective and inflammatory colitis, endoscopic intervention is required.Options are sigmoidoscopy or Colonoscopy, ideally flexible, should be perfomed to view the colonic mucosa and take biopsies to detect inflammatory changes in the colon. Ideally colonoscopy should not be performed when the disease is not in the active stage of the disease, should be performed when the patient is hemodynamically stable and the episodes of bloody diarrhea have been reduced to a minimum by medical management Colonoscopic appearance in ulcerative colitis will be shown in the following slide:
On endoscopy ulcerative colitis will be differentiated from crohn’s colitis by the facts that crohn’s disease has skip lesions in the gut and mostly causes cobblestoning and stricturing. Endoscopic appearance in crohn’s disease will be as following:
ULCERATIVE COLITIS Defined as a relapsing remitting ulcero-inflammatory disease mostly involving the large gut. CROHN’S DISEASE Defined as a relapsing remitting disease which can involve any part of the gut, mostly the small gut, characterised by transmural non-caseating granulomatous inflammation.
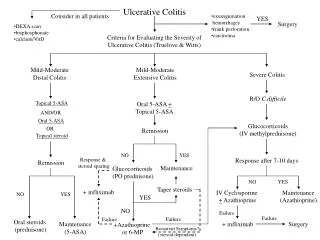
Medical management • Ulcerative colitis can be divided according to extent of involvement of the colon. The divisions are as: • Distal colitis ( Proctitis and proctosigmoiditis ) and • Extensive colitis or pan-colitis The management differs according to the extent of the disease. Treatment options include: 1. Steroids ( local, oral and parenteral ) 2. Aminosalicylates ( local and oral ) 3. Immunosuppressive therapy 4. Supportive management • According to recommendations drugs of choice for INDUCTION of remission are corticosterioids, aminosalicylates have role in induction only in high doses.
Management according to severity ACTIVE DISEASE: • MILD DISEASE ( less than 4 motions/day ) Mild disease involving only the rectum or sigmoid can be treated with steroid or aminosalicylate enemas, and oral steroids ( prednisolone 20 mg/day ) can also be added if local treatment bears no response. In colonic involvement more than the sigmoid, oral prednisolone in doses of 20-40 mg/day is given along with enemas of hydrocortisone or 5-ASA. • MODERATELY SEVERE DISEASE ( More than 4 motions/day ): These are patients who are systemically well, they should be put on oral prednisolone 40-60 mg/day and treatment should be continued for 3-4 weeks. Tapering of steroids should always be done. 5-ASA analogues are used consistently, sustained release mesalamine is available by the name of Asacol ( 2.0 -4.0 g/day ) • SEVERE DISEASE ( More than 6 bloody motions/day and systemically unwell ) These are the patients who have more than 6 motions per day and have continuously high grade fever, tachycardia and anemia. The treatment includes: a. Making the patient NPO and monitor input output b. I/V fluids and parenteral nutrition if required in malnourished c. I/V Hydrocortisone 100 mg per 6 hours or Methylprednisolone 40-60 mg/day I/V d. Abdomen should be examined for any tenderness and abdominal distention, and immediate surgical consult should be asked for. e. If despite i/v steroids, the pulse rate rises and abdomen tenderness increases along with fever persistently above 100 F, and the duration of therapy exceeds a week, then the patient is a candidate for surgery ( colectomy and ileo anal pouch fashioning ).
If there is response to i/v steroids i.e decrease in bloody motions and diminished systemic toxicity, then patient can be put on oral steroids 40mg/day. If patient does not show rapid response to i/v steroids, then addition of I/V cyclosporin in infusion 4mg/kg can be added along with steroids. It will induce remission in 60-80% of non-responsive patients.
Indications for Surgery • Intractable disease ( unresponsive to i/v steroids and immunosuppressants ) • Fulminant disease • Toxic megacolon • Colonic perforation • Massive colonic hemorrhage • Severe extra colonic manifestations
CHRONIC DISEASE: • Patients who relapse when steroids are tapered off or require 10-15 mg per day have shown good response with azathioprine 2-5 mg/kg ( being used extensively in the uk ) or mercaptopurine. These drugs allow for the gradual reduction of dose of steroids. • Oral cyclosporin 5mg/kg is also being used but no formal trials have been performed • High dose oral steroids on alternate days is also being used
Maintenance of remission • Sulphasalazine which consists of a aminosalicylate and a sulfapyridine moeity.Sulfapyridine serves as an antibiotic and together they have proved to be effective in maintaining remission when used over a a period of years. Side effects occur due to the sulfapyridine group. • OTHER OPTIONS: Infliximab which is a anti-TNF agent, is approved in the US for moderate to severe colitis, in acute settings when not responsive to i/v steroids and also when steroid tapering is required without flares. Dose is 5 mg/kg in 3 dose regimen at 0, 2 and 6 weeks in moderate to severe disease. A single dose of 5mg/kg infusion in acute severe colitis has also shown results in trials. Other immunomodulating drugs used are methotrexate,
Regular screening • Patients who have a controlled disease have to have a yearly colonoscopy with biopsy to detect any dysplastic changes as it ultimately leads to CA, so timely intervention with colectomy can be done if such changes are detected.
THANK YOU FOR YOUR PATIENCE