Download
1 / 39
400 likes | 688 Vues
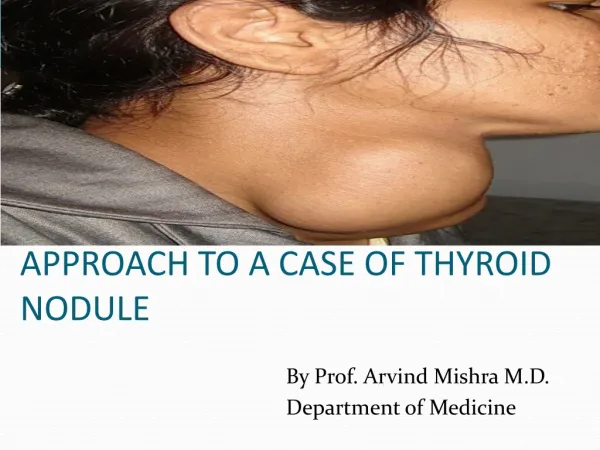
Approach to the Lumpy Thyroid Katherine A. Kovacs, MD MSc FRCPC. Setting of Thyroid Nodule Discovery. Routine neck palpation by physician Self-examination by patient Incidental finding during radiological procedure. Clinical Relevance of Nodule Discovery. Potential malignancy

E N D
Approach to the Lumpy ThyroidKatherine A. Kovacs, MD MSc FRCPC
Setting of Thyroid Nodule Discovery • Routine neck palpation by physician • Self-examination by patient • Incidental finding during radiological procedure
Clinical Relevance of Nodule Discovery • Potential malignancy • Clue to underlying thyroid pathology (i.e., Hashimoto’s thyroiditis) • Potential for thyroid dysfunction • Potential for compressive symptoms
BENIGN: Colloid nodule Hashimoto thyroiditis Simple or hemorrhagic cyst Follicular adenoma Subacute thyroiditis MALIGNANT: Follicular cell-derived carcinoma Papillary Follicular Anaplastic C-cell-derived carcinoma Medullary Thyroid lymphoma Metastatic carcinoma Etiology of Thyroid Nodules
EVALUATIONHistory • Thyroid function status • Associated pain • Compressive symptoms/Cosmetic • Establish risk factors for malignant disease • age < 30 or > 60; male sex • exposure to ionizing radiation • family history • rapid growth
EVALUATIONPhysical Examination • Number, size & consistency of lumps • Mobility • Tenderness • Presence of lymphadenopathy • Compressive signs
EVALUATIONTSH • Low-normal or suppressed TSH (< 0.5) • autonomous nodule(s) • overt hyperthyroidism indication for radioisotope scan (hot nodule, especially by I123, almost always benign) • High-normal or elevated TSH • Hashimoto’s thyroiditis • Overt hypothyroidism higher risk of malignancy
EVALUATIONUltrasound • Most sensitive test to detect thyroid nodules and recommended for all patients identified to have one or more thyroid nodules • Assess size & number of nodules • Assess for sonographic characteristics that are higher risk for malignancy • Select nodule(s) for biopsy • Accuracy dependent on expertise
MNG vs Solitary Nodule • Risk of cancer is the same in MNGs vs glands with solitary nodule • Selection for FNA should be based on U/S features rather than on size or clinically “dominant” nodules
EVALUATIONConsider Other Radiology • Technetium or I123 scan • most nodules are cold; AVOID as a routine • useful when suspecting hot nodule (low TSH) • CT thyroid/chest • useful in assessing retrosternal goitre
Indications for U/S-guided FNA • Palpation-guided FNA non-diagnostic • Complex (solid/cystic) nodule • Palpable small nodule (< 1.5 cm) • Impalpable incidentaloma • Abnormal cervical nodes • Nodule with suspicious U/S features
MANAGEMENTTreatment/Surveillance • Toxic Adenoma/MNG • surgery, high-dose RI or alcohol/laser ablation • Follicular Neoplasm • surgery for definitive diagnosis or close F/U • Carcinoma • surgery, RI PRN, & T4 suppress to TSH < 0.1 • Others • palpation, TSH, ?ultrasound, rebiopsy PRN • controversial: T4 suppression to TSH 0.1-0.4
Unanswered Questions • Sufficient length of time to follow a nodule and maximum growth allowed to conclude that it is benign
Case 1: Toxic Adenoma • 32-yr-old female manager of music store • c/o 2-3 yrs panic attacks, palpitations; 1 yr goitre, irregular menses, insomnia; 6-8 mo fatigue, muscle weakness; few weeks hand tremor, weight gain • medications: none • no FH thyroid cancer
Case 1 (cont’d) • O/E: • normal weight, BP 138/70, HR 110 (regular) • easily visible goitre with ovoid mass in L lobe (4x normal size lobe); R lobe slightly palpable with tiny nodule • hands warm and sweaty • proximal muscle weakness
Case 1 (cont’d) • Investigations: • TSH < 0.05, FT4 46 (Jan. 19) • Nuclear thyroid scan: 4.3 x 3 cm ovoid mass in L lobe with markedly increased uptake; mostly absent uptake in R lobe; 24 hr thyroid uptake 36 % (Feb. 2) • TSH 0.03, FT4 53.3, HCG < 0.5 (when I saw Mar. 19)
Case 1 (cont’d) • Treatment: • high-dose radioiodine • Response: • marked shrinkage • induction of biochemical hypothyroidism
Case 2: Multinodular Goitre • 34-yr-old taxi driver • large goitre x 9 years, gradual enlargement • pressure sensation when supine, nocturnal dry cough, frequent choking • mild fatigue, tendency to heat intolerance, gaining weight • medications: none • no FH thyroid disease
Case 2 (cont’d) • O/E: • moderately overweight, BP 148/92, HR 90 (regular) • easily visible irregular goitre, roughly 8x normal size • hands very warm
Case 2 (cont’d) • Investigations: • TSH 0.2, FT4 15.8 • U/S: diffusely enlarged heterogeneous thyroid
Case 2 (cont’d) • Treatment: • high-dose radioiodine 29 mC on 3 occasions • Response: • modest shrinkage • induction of biochemical hypothyroidism
Case 3: Colloid Nodule • 54-yr-old male chief of security • lump in thyroid detected at routine physical • no compressive symptoms • no symptoms of thyroid dysfunction • no hx significant radiation exposure • no FH thyroid cancer; mom - goitre
Case 3 (cont’d) • O/E: • mildly overweight, BP 160/92, HR 75 (regular) • easily visible, mobile L thyroid mass • no lymphadenopathy • clinically euthyroid
Case 3 (cont’d) • Investigations: • TSH 1.27 • U/S: solitary 3.4 cm inferior L thyroid nodule • Nuclear thyroid scan: solitary cold nodule • FNA x 3: unsatisfactory (cyst contents, inflammatory cells, few epithelial cells) • shrunk after procedure • U/S-guided FNA: cyst contents, fragment of thyroid tissue with normal-looking follicles • repeated after nodule grew - colloid nodule
Case 4: Follicular Neoplasm • 46-yr-old woman on disability • incidental thyroid nodule detected during CT pulm/angio for pulmonary emboli • dysphagia to liquids & solids • irritability, weight gain, fatigue, constipation • no history of significant radiation exposure • no FH thyroid cancer
Case 4 (cont’d) • O/E: • moderately overweight, BP 120/68, HR 60 (regular) • easily visible, mobile R thyroid mass • no lymphadenopathy • clinically euthyroid
Case 4 (cont’d) • Investigations: • TSH 1.11 • U/S: solitary 3.8 cm R complex thyroid nodule • FNA: few groups of follicular epithelial cells favouring neoplasm or colloid nodule • Pathology on resection: follicular adenoma