Download
1 / 64
640 likes | 834 Vues
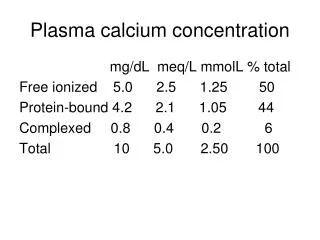
Abraxane ® (paclitaxel protein-bound particles for injectable suspension). Each 50 mL vial contains 100 mg of paclitaxel and 900 mg of human albumin as a sterile lyophilized powder. Abraxis BioScience, Inc. Approved Indication:.

E N D
Abraxane ®(paclitaxel protein-bound particles for injectable suspension). Each 50 mL vial contains 100 mg of paclitaxel and 900 mg of human albumin as a sterile lyophilized powder.Abraxis BioScience, Inc.
Approved Indication: “ABRAXANE® is indicated for the treatment of breast cancer after failure of combination chemotherapy for metastatic disease or relapse within 6 months of adjuvant chemotherapy. Prior therapy should have included an anthracycline unless clinically contraindicated.” The application was approved on January 7, 2005.
Sponsor’s Proposed Indication: “ABRAXANE® is indicated for the adjuvant treatment of node-positive breast cancer administered sequentially to standard doxorubicin-containing combination chemotherapy."
Regulatory Pathways to Market a Competitor Drug • NDA • ANDA • 505(b)(2)
505(b)(2) • This applies to new formulations of marketed drugs and authorizes the FDA, where appropriate, to base approvals of new drugs entirely or partially on studies not conducted by the applicant and for which the applicant has not obtained a right of use.
505(b)(2) Criteriafor Abraxane in Metastatic Breast Cancer • FDA agreed to use the preclinical genetic toxicology studies from the Taxol application to support Abraxane approval • FDA also agreed to use response rate as a comparative measure of Taxol antitumor activity instead of the more stringent standard time to event endpoint.
Presentation Outline • Abraxis proposal for approval of Abraxane for the new adjuvant indication • Pharmacokinetics of Abraxane • Abraxane’s basis of approval for metastatic breast cancer • Taxol’s basis of approval for adjuvant breast cancer • FDA concerns with Abraxis proposal • Statistical plan to approve Abraxane in the adjuvant breast cancer setting • Questions to ODAC Committee
Abraxis proposal for approval of Abraxane • Results of the randomized Intergroup study that served as the basis for Taxol approval for the adjuvant treatment of node positive early breast cancer. • Preclinical genetic toxicology studies with Taxol.
Abraxis proposal for approval of Abraxane (continued) • Comparison of the pharmacokinetics of the Abraxane and Taxol paclitaxel formulations. • Results of the study comparing Abraxane and Taxol that served as the basis for approval of Abraxane for metastatic breast cancer. • Study CA030, a single arm 30 patient study of dose dense AC q 2 weeks x 4 cycles followed by dose dense Abraxane 260 mg/m2 q 2 weeks x 4 cycles.
Abraxis proposal for approval of Abraxane (continued) • March 13, 2006: single arm phase II safety study to support the approval of adjuvant breast cancer • July 2006:proposal for a 400 patient randomized safety study comparing Abraxane and Taxol in adjuvant treatment of node positive early breast cancer to be conducted prior to approval. • August 9, 2006: changed to a post approval Phase 4 safety study of unspecified size.
Is Abraxis proposal acceptable? • How similar or dissimilar the Abraxane and Taxol formulations are. • Risk/benefit ratio of approving Abraxane w/o an efficacy and safety study. • Taxol prolongs disease free survival and survival in the adjuvant breast cancer setting. • FDA is concerned with the consequences of a potential decrement in DFS and survival in women with node positive early breast cancer.
A Pharmacokinetic Comparison of Abraxane and Taxol Brian Booth Division of Clinical Pharmacology 5
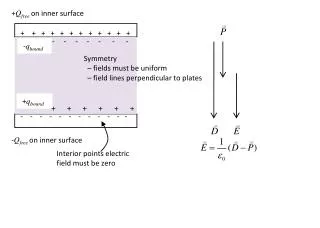
PK Comparison-Paclitaxel moieties Albumin P P P P Total Paclitaxel P P P In vivo Abraxane Paclitaxel P P P P Total Paclitaxel P P P P P P In vivo Taxol
PK Comparison-Paclitaxel moieties • Conventional thinking about drug action • Free drug mediates effect • Abraxane: Total Paclitaxel= • Taxol: Total Paclitaxel= • Taxol, Abraxane • How much free paclitaxel is generated by each? • Unknown • Comparative biodistribution of paclitaxel from Abraxane and Taxol in patients? • Unknown P P P P
PK Comparison-LinearityTotal Paclitaxel Abraxane: 30 min infusion Linear, predictable PK Taxol: 3 hr infusion Non-linear, less-predictable PK
Clinical PK Comparison of Abraxane and Taxol- Study C008-0 Total Paclitaxel • PK study- • Abraxane 14 patients • Taxol 12 patients • Comparability issues • Different Doses • Abraxane 260 mg/m2 • Taxol 175 mg/m2 • TOTAL Paclitaxel
Clinical PK Comparison of Total PaclitaxelStudy C008-0-UnadjustedTotal Paclitaxel Abraxane: 6.5 x higher Cmax 17 % higher AUC 40% higher CL 50% higher Vd Than Taxol Taxol (175 mg/m2) Abraxane (260 mg/m2) Sparreboom A. et al Clin Cancer Res 2005; 11:4136-4143
Clinical PK Comparison of Total PaclitaxelStudy C008-0 Abraxane (dose-adjusted to 175 mg/m2) Taxol (175 mg/m2)
Dose-normalized comparisonof Abraxane and Taxol *Dose-normalized. Abraxane is a 30-minute infusion; *Taxol is a 3-hr infusion
Summary • Abraxane and Taxol are not pharmacokinetically “the same” (Total paclitaxel) • Need to assess free paclitaxel concentrations • Different doses • Different CL • Different Vd • Different AUC • Different Cmax • Abraxane linear PK, Taxol non-linear PK
Study Design • Randomized, Phase 3, open label • Sample size: 460 patients • 70 sites: Russia (77%), UK (15%), Canada and US (9%) • 2 Arm: Abraxane 260 mg/m2 as a 30-minute infusion and Taxol 175 mg/m2 as a 3-hour infusion • 59% second line or greater and 77% previous anthracycline exposure • Designed to show non inferiority in RR
Study Populations • All randomized patients • Subgroups • Receiving drug as 1st line only • Receiving drug as > 2nd line • Taxol approved indication: patients who have failed combination chemotherapy for metastatic disease or relapse within 6 months of adjuvant chemotherapy. Prior therapy should have included an anthracycline unless clinically contraindicated
Endpoints • 1° Endpoint: Response Rate • 2° Endpoints: TTP Survival
TTP At the time of Abraxane approval TTP results were not included in the label because: Evaluation of TTP was not rigorous and data were not sufficiently mature to support a comparative efficacy claim in this single non-blinded study
Time to progression (TTP) from July 21, 2006 Submission We have the following concerns: • TTP was not systematically assessed in all patients after cycle 6 • Multiple analyses using different criteria without adjustments • TTP results may not be reliable for a labeling claim
Overall Survival from July 21, 2006 Submission We have the following concerns: • There was no difference in overall survival between the Abraxane and Taxol treatment groups. HR (Abraxane/Taxol) was 0.90, p=0.348 (log rank). • No conclusions can be drawn from a subgroup analysis when the main analysis was not statistically significant. • Multiple subgroup analyses using different criteria without p value adjustments • P-values are not interpretable
Disease Free Survival: AC vs AC+T(HR=0.78, 95% CI 0.67-0.91, p=0.0022)
Survival: AC versus AC+T (HR=0.74, 95% CI 0.60-0.92, p=0.0065)
Disease Free Survival: AC vs AC+T Receptor Neg/Unknown(HR=0.68, 95% CI 0.55-0.85)
Should Abraxane be approved for the adjuvant treatment of node positive early breast cancer without an adequate RCT powered for DFS, OS and safety?
Abraxane and Taxol are different • Formulations are different • Pharmacokinetics are different • Not bioequivalent • Free paclitaxel not measured • Abraxane does not contain cremophor, given by 30 minute infusion w/o premedication • Taxol is given by 3 hour infusion and requires premedication
Abraxane and Taxol toxicity profiles are different • Taxol has a higher incidence of neutropenia and hypersensitivity reactions • Abraxane has a higher incidence of peripheral neuropathy, nausea, vomiting, diarrhea and asthenia
FDA Agrees that in the metastatic breast cancer studyAbraxane had a higher tumor response rate than Taxol
FDA believes that in the MBC study TTP improvement has not been adequately demonstrated • There was no type 1 error allocated for TTP analysis. • TTP claims could not be confirmed since no IRL review was conducted beyond cycle 6. Patients were not systematically evaluated after cycle 6. In an open label study, there is a potential for bias in progression assessments. • P-values for TTP analyses are not interpretable.
FDA believes that in the MBC study survival improvement has not been adequately demonstrated • There was no type 1 error allocated for OS analysis. • There is no significant OS effect in the all randomized population • Subgroup analysis is not appropriate when the study failed to demonstrate an effect in the overall population. • Multiple analyses in multiple subgroups with no adjustment • P-values for OS analyses is not interpretable.
1st line patients, survival trended against Abraxane HR (A/T)= 1.215
There is a need for a RCT in the adjuvant population to properly estimate the risk:benefit ratio of Abraxane
Data on toxicity comparisons from the metastatic study may not be appropriate to the adjuvant setting were Abraxane would be given following AC.
Taxol increases DFS and OS in the adjuvant treatment of women with node positive early breast cancer. • 22% reduction in the risk of disease recurrence • 26% reduction in the risk of death
FDA is concerned with the consequences of a potential decrement in DFS and survival in women with node positive early breast cancer
Trial Design Considerations R. Sridhara, Ph.D.