Download
1 / 4
40 likes | 149 Vues
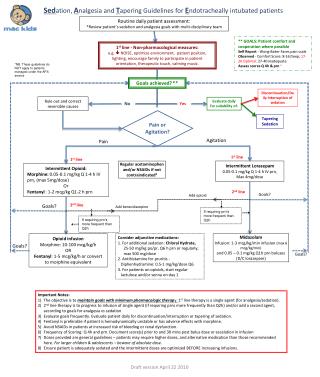
This document outlines essential protocols for sedation and analgesia management in endotracheally intubated patients. It emphasizes multi-disciplinary assessments to optimize patient comfort and cooperation, using both observational and self-reporting pain scales. First-line non-pharmacological measures and a systematic approach to tapering sedation are discussed, including regular evaluations and adjustments based on patient goals. The guidelines also address the management of withdrawal risks and establish protocols for intermittent medications, with emphasis on individualized patient care strategies.

E N D
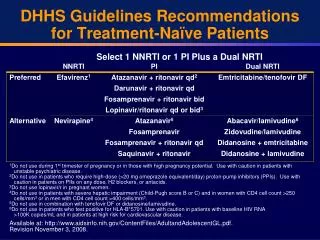
Sedation, Analgesia and Tapering Guidelines for Endotracheally intubated patients Routine daily patient assessment: *Review patient’s sedation and analgesia goals with multi-disciplinary team ** GOALS: Patient comfort and cooperation where possible Self Report - Wong-Baker Faces pain scale Observed - Comfort Score: 8-16 Deep; 17-26 Optimal; 27-40 inadequate Assess scores Q 4h & prn 6 1st line - Non-pharmacological measures: e.g. NOISE, optimize environment, patient position, lighting, encourage family to participate in patient orientation, therapeutic touch, calming music. *NB. These guidelines do NOT apply to patients managed under the APS service Goals achieved?** Discontinuation/Daily Interruption of sedation Rule out and correct reversible causes Evaluate daily for suitability of: No Yes Pain or Agitation? Tapering Sedation Agitation Pain 1st line 1st line Intermittent Lorazepam 0.05-0.1 mg/kg Q 1-4 h IV prn, Max 4mg/dose Regular acetaminophen and/or NSAIDs if not contraindicated5 Intermittent Opioid: Morphine: 0.05-0.1 mg/kg Q 1-4 h IV prn, (max 5mg/dose) Or Fentanyl: 1-2 mcg/kg Q1-2 h prn 2nd line Goals? Add opioid Goals? 2nd line Add benzodiazepine If requiring prn’s more frequent than Q2h If requiring prn’s more frequent than Q2h Opioid infusion Morphine: 10-100 mcg/kg/h OR Fentanyl: 1-5 mcg/kg/h or convert to morphine equivalent Consider adjunctive medications: 1. For additional sedation: Chloral Hydrate, 25-50 mg/kg po/pr, Q6 hprn or regularly; max 500 mg/dose Antihistamine for pruritis -Diphenhydramine: 0.5-1 mg/kg/dose Q6 For patients on opioids, start regular lactulose and/or senna on day 1 Midazolam Infusion: 1-3 mcg/kg/min infusion (max 6 mcg/kg/min) and 0.05 – 0.1 mg/kg Q1h prn boluses (D/C lorazepam) Goals? Goals? Important Notes: • The objective is to maintain goals with minimum pharmacologic therapy. 1st line therapy is a single agent (for analgesia/sedation). • 2nd line therapy is to progress to infusion of single agent (if requiring prns more frequently than Q2h) and/or add a second agent, according to goals for analgesia vs sedation • Evaluate goals frequently. Evaluate patient daily for discontinuation/interruption or tapering of sedation. • Fentanyl is preferable if patient is hemodynamically unstable or has adverse effects with morphine. • Avoid NSAIDs in patients at increased risk of bleeding or renal dysfunction. • Frequency of Scoring: Q 4h and prn. Document score(s) prior to and 30 mins post bolus dose or escalation in infusion • Doses provided are general guidelines – patients may require higher doses, and alternative medication than those recommended here. For larger children & adolescents – beware of absolute dose. • Ensure patient is adequately sedated and the intermittent doses are optimized BEFORE increasing infusions. Draft version April 22 2010
Daily Interruption of Sedation (DIS) and Tapering Guidelines 1st line: non-pharmacological measures, rule out reversible causes of agitation/pain * Individualize Patient Goals Higher risk of withdrawal ( > 5 -7 days continuous IVI/ high cumulative dose) Lower risk of withdrawal (≤ 5 days continuous IVI) Initiate WAT scoring yes yes Institute DIS** Q am: Hold all IVI sedative infusions. Continue intermittent sedatives as needed Reduce IVI rate by 50% (you may drop to this dose at once, or wean over 1st 24h) 3Wean IVI by 20% of baseline rate Q4-24h as tolerated End-points (any 1 of the following): • ≥ prns in 3 h • 1WAT-1 > 3 • Cardioresp instability • Ventilator dysynchrony yes Patient is in withdrawal Despite prn dose(s) yes Administer prn doses benzo/opioid to treat symptoms Consider delirium and/or sleep disorder Resume IVI sedative infusion(s) at 50% original rate. Adjust dose to achieve patient goals. Resume/Increase background infusion rate by 20%/more to achieve target ** Patient is not eligible for DIS if: • Currently receiving muscle relaxants • Risk of withdrawal. • Continuous IVI sedation for any of the following: seizure control, ICP control, palliative/comfort care, active cooling protocol • Baseline persistent (not periodic) discomfort/agitation WAT-1 score ≤ 3 or patient requires < 4 prn doses/day Important notes: • 1 If patient is at risk of withdrawal, initiateWAT-1 scoring Q 4 hrly and prn until < 3 xs 2 • 2Weaning dose range: 10-50% of peak dose Q4-24h • 3Individualize duration of taper • 41st line, non-pharmacological. For delirium: Chlorpromazine: 0.5-1 mg/kg IV q6h prn (initial max 25 mg/dose). For sleep disorder: consult MRP & PCCU pharmacist yes Resume tapering algorithm Draft version April 22 2010
Comfort Scale: (Score after a 2 min period of observation) fre PAIN Scales: use to supplement the COMFORT scale, in patients who are cognitively and physically able to respond (e.g. age ≥ 3 years) Draft version April 22 2010
DAILY INTERRUPTION OF SEDATION (DIS) What is DIS = focused downward titration of sedatives over time Objectives: daily “wake-up”; minimize pharmacological intervention and prevent adverse events; optimise patient outcomes Rationale: DIS in adults has been shown to facilitate spontaneous breathing, and has been associated with decreased mortality, hospital stay, withdrawal and delirium, improved ventilator free days and psychological outcomes Patient is not eligible for DIS if: • Currently receiving muscle relaxants • Risk of opioid/sedation withdrawal. • Continuous IVI sedation for: • seizure control • ICP control • palliative/comfort care • active cooling protocol • Baseline persistent (not periodic) discomfort/agitation Draft version April 22 2010