VESTIBULAR DISORDERS
VESTIBULAR DISORDERS. Joannalyn B. Juego. ANATOMY: Peripheral Vestibular System. Stabilizing the visual images on the fovea of the retina during head movements to allow clear vision Maintaining postural stability Providing information used for spatial orientation.

VESTIBULAR DISORDERS
E N D
Presentation Transcript
VESTIBULAR DISORDERS Joannalyn B. Juego
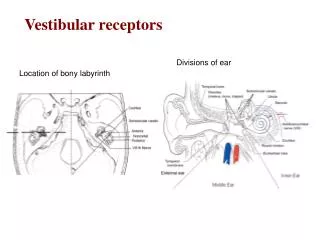
ANATOMY: Peripheral Vestibular System • Stabilizing the visual images on the fovea of the retina during head movements to allow clear vision • Maintaining postural stability • Providing information used for spatial orientation
ANATOMY: Peripheral Vestibular System • Semicircular canals • Otolith organs • Central vestibular system
Vestibular System Dysfunction • Peripheral Pathology • Central Nervous System Pathology
Peripheral Pathology: Mechanical • BPPV • Most common cause of vertigo • A biomechanical disorder • Nystagmus & vertigo without change in head position; nausea with or without vomiting; & dysequilibrium • Latency to onset of the vertigo & nystagmus occurs within 15 seconds once the head is in the provoking position; the duration is less than 60 seconds
Cupulolithiasis • Fragments of the otoconia break away & adhere to the cupula of one of the SCCs • When the head is moved into certain positions, the weighted cupula is deflected by the pull of gravity • The abnormal signal results in vertigo & nystagmus, which persists as long as the patient is in the provoking position
Canalithiasis • Otoconia are freely floating in one of the SCCs • When a patient changes head position, the pull of gravity causes the freely floating otoconia to move inside the SCC resulting in endolymph movement & deflection of the cupula
Peripheral Pathology: Decreased Receptor Input • UVH • Viral insults, trauma, & vascular events • Vertigo, spontaneous nystagmus, oscillopsia during head movements, postural instability, & dysequilibrium • Resolves within 3-7 days assuming the patient is exposed to common daylight conditions
Peripheral Pathology: Decreased Receptor Input • BVH • Ototoxicity • Meningitis, autoimmune DO, head trauma, tumors on the 8th CN, transient ischemic episodes of vessels supplying the vestibular system, & sequential unilateral vestibular neuronitis • Dysequilibrium, oscillopsia, & gait ataxia
Central Nervous System Pathology • Cerebrovascular insults involving the AICA, PICA, & vertebral artery • Vertebrobasilar insufficiency (VBI) • TBI due to labyrinthine or skull fractures • Demyelinating diseases such as MS affecting CN VIII
PHYSICAL THERAPY EXAMINATION • History & Systems Review • Identification of symptoms • Duration & circumstances of symptoms
Identification of Symptoms • Dizziness • Vaguely defined as the sensation of whirling or feeling a tendency to fall • Patients should be directed away from using the word & to use more precise terms • Vertigo, lightheadedness, dysequilibrium, oscillopsia
Vertigo • Illusion of movement • Episodic • Indicates pathology at one or more locations along the vestibular pathways • Acute stage of UVH • Displaced otoconia (BPPV) • Acute unilateral brainstem lesion
Lightheadedness • Feeling that fainting is about to occur • Causes • Orthostatic hypotension • Hypoglycemia • Anxiety • Panic disorder
Dysequilibrium • Sensation of being off balance • Causes • BVH • Chronic unilateral vestibular hypofunction • Lower extremity somatosensation loss • Upper brainstem/vestibular cortex lesion • Cerebellar & motor pathway lesions
Oscillopsia • Subjective experience of motion of objects in the visual environment that are known to be stationary • Occur with head movements in patients with vestibular hypofunction since the vestibular system is not generating an adequate compensatory eye velocity during the head motion
Duration & Circumstances of Symptoms • How recent the attacks happened • Whether the symptom is constant or episodic • Episodic: average duration of the episodes • Seconds to minutes – BPPV • Minutes to hours – Meniere’s disease • Days – vestibular neuronitis or migraine-associated dizziness
Duration & Circumstances of Symptoms • Whether the patient experiences symptoms with particular movements, positions, or at rest • Is the patient sensitive to motion as the passenger in a moving car? • Does the patient experience a vigorous vertigo when the head is moved into certain positions?
Tests & Measures • Visual Analogue Scale • Dizziness Handicap Inventory • Functional Disability Scale • Vestibular Rehabilitation Benefit Questionnaire • Motion Sensitivity Quotient • Examination of Eye Movements
Observation for Nystagmus • Nystagmus is the primary indicator used in identifying most peripheral & central vestibular lesions • The direction of the nystagmus is named by the direction of the fast component • Left beating nsytagmus: eyes move slowly to the right & the resetting eye movement is to the left
Head Impulse Test (Examination of the VOR at High Acceleration) • Widely accepted clinical tool used to examine semicircular canal function • Patient first fixates on a near target • When testing the horizontal SCC, the head is flexed to 30 deg
Head Impulse Test (Examination of the VOR at High Acceleration) • Patient is asked to keep their eyes focused on a target while his head is manually rotated in an unpredictable direction using a • Small amplitude (5 – 15 deg), • Moderate velocity (~200 deg/sec), and • High-acceleration (3,000 – 4,000/sec) angular impulse
Head Impulse Test (Examination of the VOR at High Acceleration) • Normal • Eyes will move in the direction opposite to the head movement & gaze will remain on the target • With a loss of vestibular function • The VOR will not move the eyes as quickly as the head rotation & the eyes will move off the target • The patient will then make a corrective saccade to reposition the eyes on the target • Corrective saccade: rapid eye movement used to reposition the eyes to the target of interest
Head Impulse Test (Examination of the VOR at High Acceleration) • Unilateral peripheral lesion or pathology of the central vestibular neurons • Patient will not be able to maintain gaze when the head is rotated quickly toward the side of the lesion • Bilateral loss of vestibular function • Patient will make corrective saccades after a head impulse to either side
Head-Shaking Induced Nystagmus Test (HSN) • Useful aid in the diagnosis of a unilateral peripheral vestibular defect • Patient is instructed to close his eyes • Clinician flexes the head 30 deg before oscillating horizontally for 20 cycles at a frequency of 2 repetitions per second • On stopping the oscillation, the patient opens the eyes & the clinician checks for nystagmus
Head-Shaking Induced Nystagmus Test (HSN) • Normal • Nystagmus will not be present • Presence of asymmetry between the peripheral vestibular inputs to central vestibular nuclei • May result in HSN • UVH • Horizontal HSN • Quick phases of the nystagmus directed toward the healthy ear & the slow phases directed toward the lesioned ear
Positional Testing • Commonly used to identify whether otoconia have been displaced into the SCC, causing a condition referred to as Benign Paroxysmal Positional Vertigo (BPPV) • Dix-Hallpike Test • Patient is moved from a long-sitting position with the head rotated 45 deg to one side, to a supine position with the head extended to 30 deg beyond horizontal, head still rotated to 45 deg • Observe the eyes for nystagmus
Positional Testing • Dix-Hallpike Test Side-lying • Patient sits on the edge of the examination table • Clinician turns the head horizontally 45 deg • Patient is quickly brought down to the side opposite the head rotation • Examiner checks for nystagmus & vertigo, & then slowly brings the patient to the starting position • The other side is then tested
Positional Testing • Roll test • If horizontal SCC BPPV is suspected • Patient is positioned supine with the head flexed 20 deg • Rapid rotations to the sides are done separately & the clinician observes for nystagmus & vertigo
Dynamic Visual Acuity (DVA) Test • Measurement of visual acuity during horizontal motion of the head • Static visual acuity is first determined • Patient is asked to “Read the lowest line you can see” on a wall-mounted acuity chart • Lighthouse ETDRS (Early Treatment Diabetic Retinopathy Study) wall charts are recommended • Patient then attempts to read the chart while the clinician horizontally oscillates the patient’s head at a frequency of 2Hz
Dynamic Visual Acuity (DVA) Test • Normal • Head movement results in little or no change of visual acuity compared with the head still (less than 1 line difference) • Loss of vestibular function • Eyes will not be stable in space during head movements • Decrement in DVA compared with visual acuity when the head is still • A 3-line or more decrement in visual acuity during head movement is suggestive of vestibular hypofunction
Vestibular Function Tests: Semicircular Canal Tests • Electronystamography (ENG) & Videonystamography (VNG) • Oculomotor & inner ear function • Rotational chair test • Rotating subjects in the dark • Standard test for bilateral vestibular dysfunction
Vestibular Function Tests: Otolith Tests • Vestibular-evoked myogenic potential (VEMP) • Cervical VEMP • Ocular VEMP
Benign Paroxysmal Positional Vertigo • The otoconia will be returned into the vestibule • The patient will demonstrate reduced vertigo associated with head motion • The patient will demonstrate improved balance • The patient will demonstrate independence in ADLs
Benign Paroxysmal Positional Vertigo • Canalith repositioning maneuver (CRM) • BPPV due to canalithiasis, posterior SCC canalithiasisis the most common • Liberatory (Semont) maneuver • BPPV due to cupulolithiasis, posterior SCC cupulolithiasis is the most common • Brandt-Daroff exercises • Persistent/residual or mild vertigo (even after CRM); for the patient who may not tolerate CRM
Unilateral Vestibular Hypofunction • The patient will demonstrate improved stability of gaze during head movement • The patient will demonstrate diminished sensitivity to motion • The patient will demonstrate improved static & dynamic postural stability • The patient will be independent in proper performance of a HEP that includes walking
Unilateral Vestibular Hypofunction • Gaze Stability Exercises • Improve the VOR & other systems that are used to assist gaze stability with head motion • Designed to expose patients to retinal slip
Retinal Slip • Occurs when the image of an object moves off the fovea of the retina, resulting in visual blurring • Necessary as this is the signal used to drive vestibular adaptation within the brain • Because the brain can tolerate small amounts of retinal slip yet see a target clearly, the patient must try to keep the target in focus • Otherwise, head motion that is too rapid will result in excessive retinal slip
Primary Paradigms of Vestibular Adaptation • x1 exercises • Patient is asked to move the head horizontally as quickly as possible while maintaining focus on a stable target • Patient must learn how to slow the head movement if the target becomes blurred • Starting target distance should be an arm’s length away
Primary Paradigms of Vestibular Adaptation • x2 exercises • Requires the patient to move the head & the target in opposite directions