Meningococcal Disease
Neisseria meningitidis. Meningococcal Disease. MKT4734 1/1/99. Neisseria meningitidis. Etiology. Gram negative diplococcus with polysaccharide capsule 13 serogroups classed by capsular specificity (A/B/C/Y/W-135 & others) T-independent capsular antigen (no memory response)

Meningococcal Disease
E N D
Presentation Transcript
Neisseria meningitidis Meningococcal Disease MKT4734 1/1/99
Neisseria meningitidis Etiology • Gram negative diplococcus with polysaccharide capsule • 13 serogroups classed by capsular specificity (A/B/C/Y/W-135 & others) • T-independent capsular antigen (no memory response) • Other classifications - outer membrane proteins & lipopolysaccharide (LPS) 1. Apicella MA, Chapter 189: Neisseria meningitidis. In: Principles and Practice of Infectious Diseases, 4th ed. Eds. Mandell GL, et al. Churchill Livingstone, New York, 1995, 1896-1898
Antigens & VirulenceFactors Etiology Porin* (PorA or PorB) Polysaccharide Capsule Opacity* Associated Protein (Opa) Pili LPS * outer membrane proteins 10. Poolman JT, Development of a meningococcal vaccine, Infectious Agents and Disease, 4:1, 1995, 21
Neisseria meningitidis Epidemiology • Incubation - 2 to 10 days; often 3 to 42 • Transmission2 - • respiratory route • direct contact • Reservoir - humans only10 • Carrier prevalence - 5% to 10%10, 14 2. WHO Information Fact Sheets, Meningococcal meningitis-Update: http://www.who.int/inf-fs/en/fact105.html 10. Poolman JT, Development of a meningococcal vaccine, Infectious Agents and Disease, 4:1, 1995, 13 14. Herf C, et al, Meningococcal disease: recognition, treatment, and prevention, The Nurse Practitioner, 23:8, 1998, 33
Global Epidemiology Epidemiology • Group A epidemics: Senegal, Gambia, Guinea-Bissau, Guinea, Sierra Leone, Ivory Coast, Burkina Faso, Ghana, Togo, Benin, Nigeria, Cameroon, Chad, Niger, Mali, Cen. African Republic, Sudan, Uganda, Kenya, Ethiopia 4. CDC, Control and prevention of meningococcal disease and control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 4
Global Epidemiology Epidemiology • Meningitis belt - peaks in dry season • Epidemics occasionally occur in: • Saudi Arabia • Kenya & Tanzania • Burundi & Mongolia • CDC travelers information - (404) 332-4559 4. CDC, Control and prevention of meningococcal disease and control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 4
U. S. Epidemiology Epidemiology • 2100 - 3500 cases (1981-1996) and 200 - 290 deaths (1986-1995) annually23 • Highest total disease incidence in children 3 to 12 mos. of age4 • Leading cause of bacterial meningitis in ages 2 to 18 yrs.5 • Peaks late winter/early spring4 Serogroup Distribution - 1989-1991 4. CDC, Control and prevention of meningococcal disease and control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 1 5. Schuchat A, et al, Bacterial meningitis in the United States in 1995, The New England Journal of Medicine, 337:1997, 970 23. CDC. Summary of notifiable diseases, United States, MMWR 45:53, 1996,74, 76, 80
U.S. Total Disease Incidence < 5 to > 59 yrs. - 1989 -1991 Epidemiology Incidence (cases/100,000) <5 5 - 10 Age (years) 20 - 24 15 - 20 40 - 44 55 - 59 45 - 49 10 - 15 25 - 29 50 - 54 >59 35 - 39 30 - 34 4. CDC, Control and prevention of meningococcal disease and control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 2, with actual data points supplied by CDC
U.S. Total Disease Incidence < 1 to 23 mos. - 1989 -1991 Epidemiology U.S. Incidence of Meningococcal Disease < 1 to 23 Months 1989-1991 Incidence (cases/100,000) 4. CDC, Control and prevention of meningococcal disease and control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 2, with actual data points supplied by CDC
Bacterial Meningitis Incidence Major Causes Epidemiology Age (months) 5. Schuchat A, et al, Bacterial meningitis in the United States in 1995, The New England Journal of Medicine, 337:1997, 972
Meningococcal Disease United States Epidemiology • Case-fatality rate • 13% for meningitic disease (isolated in CSF)4 • 11.5% when isolated from blood4 • case-fatality rate even higher with severe meningococcemia1 • case-fatality rate consistent in spite of antibiotic use4 1. Apicella MA, Chapter 189: Neisseria meningitidis. In: Principles and Practice of Infectious Diseases, 4th ed. Eds. Mandell GL, et al. Churchill Livingstone, New York, 1995, 1899 4. CDC, Control and prevention of meningococcal disease and control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 1
U.S.A.- Changing Serogroup Prevalence - 1990’s Epidemiology • Group C common cause of outbreaks since early 1990’s6 • Group Y disease also increasing4 • Overall invasive disease incidence constant 1.3/100,000 (since 1986)5 • Meningitis incidence decreased 0.9 to 0.6/100,000 (since 1986)5 4. CDC, Control and prevention of meningococcal disease and control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 1 5. Schuchat A, et al, Bacterial meningitis in the United States in 1995, The New England Journal of Medicine, 337, 1997, 972 6. CDC, Control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 13
Serogroup C Outbreaks - United States - 1980 - 1993 Epidemiology • 21 outbreaks6 • 8 school outbreaks8 • 3 institutional outbreaks8 • 10 community outbreaks (no known contact)8 • Affect school-aged children & young adults 8 • High frequency and severity of sequelae17 • Most attack rates > 10 cases/100,000 (20 X higher than endemic rate)6 6. CDC, Control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 13 8. Jackson LA, et al, Serogroup C meningococcal outbreaks in the United States, an emerging threat, JAMA, 273:5, 1995, 384, 386 17. Erickson L, et al, Complications and sequelae of meningococcal disease in Quebec, Canada, 1990-1994, Clin Infect Dis, 26, 1998, 1163
Serogroup Y Disease - United States Epidemiology • Increasing proportion of disease since 19917 • More frequently associated with meningococcal pneumonia7 • Median age 21.8 yrs.7 7. CDC, Serogroup Y meningococcal disease - Illinois, Connecticut, and selected areas, United States, 1989-1996, MMWR, 45:46, 1996, 1010-1013 9. Quick uptakes . . . meningitis patterns shift, JAMA, 279:16, 1998, 1249
Clinical Syndromes19955 Epidemiology 5. Schuchat A, et al, Bacterial meningitis in the United States in 1995, The New England Journal of Medicine, 337, 1997, 973
Risk Groups Epidemiology • Persons with terminal complement deficiencies • Persons with anatomic or functional asplenia • Persons with immunosuppression • Industrial or laboratory personnel routinely exposed to organism • Residents or travelers to hyperendemic or epidemic areas 4. CDC, Control and prevention of meningococcal disease and control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 3 & 4
Stages of Pathogenesis Pathogenesis Organism Enters Nose or Mouth11 Mucosal Barrier Cleared11 Intravascular Space Invaded11 Host Response12 (Cytokines, PAF*, Arachidonic Metabolites) * Platelet activation factor 11. Quagliarello V, et al, Bacterial meningitis: pathogenesis, pathophysiology, and progress, The New England Journal of Medicine, 327:12, 1992, 865 12. Saez-Llorens X, et al, Molecular pathophysiology of bacterial meningitis: current concepts and therapeutic implications, The Journal of Pediatrics, 116:5, 1990, 672, 673, 675, 677
Disease Manifested Pathogenesis HostResponse12 Blood Brain Barrier Breached Effective Immune Response 1,12 13,26 1,13, 26 Meningitis with or without Meningococcemia Vascular Damage, DIC*, Tissue Damage, Shock Bacteremia without Sepsis 1,12 13,26 Meningococcemia without Meningitis * Disseminated Intravascular Coagulation 1. Apicella MA, Chapter 189: Neisseria meningitidis. In: Principles and Practice of Infectious Diseases, 4th ed. Eds. Mandell GL, et al. Churchill Livingstone, New York, 1995, 1900 12. Saez-Llorens X, et al, Molecular pathophysiology of bacterial meningitis: current concepts and therapeutic implications, The Journal of Pediatrics, 116:5, 1990, 672, 673, 675-677 13. Young LS, Chapter 56: Sepsis syndrome. In: Principles and Practice of Infectious Diseases, 4th ed., Eds. Mandell GL, et al. Churchill Livingstone, New York, 1995, 690-705 26. Glode MP, Smith AL, Meningococcal disease. In: Textbook of Pediatric Infectious Diseases. Eds. Feigin RD, et al. W. B. Saunders Company, Phila., 1981, 916 - 928
Meningococcemiawithout Meningitis Clinical Manifestations • Malaise, weakness, nausea, myalgia, arthralgia15 • Significant fever & chills15 • Macular, erythematous rash usually on extremities15 • Petechiae/purpura on extremities14,15 • Hypotension14 14. Herf C, et al, Meningococcal disease: recognition, treatment, and prevention, The Nurse Practitioner, 23:8, 1998, 33 15. Howe WB, Meningococcemia heading off a killer, The Physician and Sportsmedicine, 24:2, 1996, 2
Clinical Manifestations Meningococcemiawithout Meningitis (cont’d.) • Disseminated intravascular coagulation (DIC)14 • Multiorgan failure14 • Laboratory abnormalities15 • leukocytosis with left shift • leukopenia • coagulopathy • blood positive for N. meningitidis 14. Herf C, et al, Meningococcal disease: recognition, treatment, and prevention, The Nurse Practitioner, 23:8, 1998, 33 15. Howe WB, Meningococcemia heading off a killer, The Physician and Sportsmedicine, 24:2, 1996, 2
MeningococcemiaComplications Clinical Manifestations • Waterhouse-Friderichsen syndrome (10%)15 • Pneumonia1 • Endocarditis, myocarditis, pericarditis15 • Pleurisy15 • Peritonitis15 • Arthritis15 1. Apicella MA, Chapter 189: Neisseria meningitidis. In: Principles and Practice of Infectious Diseases, 4th ed. Eds. Mandell GL, et al. Churchill Livingstone, New York, 1995, 1902 15. Howe WB, Meningococcemia heading off a killer, The Physician and Sportsmedicine, 24:2, 1996, 2
Clinical Manifestations Expressions of Waterhouse-Friderichsen Syndrome • Fulminant septicemia • Shock • Purpura fulminans • DIC • Congestive heart failure • Bilateral adrenal hemorrhage • Progressive, irreversible collapse 15. Howe WB, Meningococcemia heading off a killer, The Physician and Sportsmedicine, 24:2, 1996, 2 25. DeLellis RA, Chapter 26: The endocrine system. In: Robbins Pathologic Basis of Disease 4th ed. Eds. Cotran RS, et al. W. B. Saunders Company, Phila., 1989, 1253
Meningitis with/withoutMeningococcemia Clinical Manifestations • Fever • Headache • Nuchal rigidity • CSF • > WBCs • < glucose • > Protein levels • + for N. meningitidis 14. Herf C, et al, Meningococcal disease: recognition, treatment, and prevention, The Nurse Practitioner, 23:8, 1998, 33
Clinical Manifestations Meningitis with/withoutMeningococcemia • Outcomes • Death • Long-term neurologic sequelae • deafness • cranial nerve palsy • retardation 14. Herf C, et al, Meningococcal disease: recognition, treatment, and prevention, The Nurse Practitioner, 23:8, 1998, 33
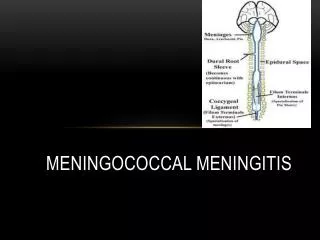
Pathogenesis - Meningitis Clinical Manifestations Skull Dura mater Capillary in arachnoid Space Brain
Clinical Manifestations Pathogenesis - Meningitis Blood Brain Barrier (Tight Junctions) Meningococci
Clinical Manifestations Pathogenesis - Meningitis 4. Neutrophils summoned; attach to endothelium 1. Meningococci release endotoxins 2. Cytokines summoned; endothelial cell inflamed 5. Neutrophils enter brain; secrete inflammatory factors; further BBB disruption 3. Blood Brain Barrier disrupted 11. Quagliarello V, et al, Bacterial meningitis: pathogenesis, pathophysiology, and progress, N Eng Jour Med, 327:12, 1992, 866-868 12. Saez-Llorens X, et al, Molecular pathophysiology of bacterial meningitis: current concepts and therapeutic implications, Journ Pediatrics, 116:5, 1990, 672, 673, 673-678
Diagnostic Features(Adults & Children) Diagnosis • Upper respiratory symptoms • Headache • Petechiae/purpura (significant finding) • Fever • Extreme vomiting • Photophobia • Nuchal rigidity 14. Herf C, et al, Meningococcal disease: recognition, treatment, and prevention, The Nurse Practitioner, 23:8, 1998, 33
Diagnostic Features(Infants) Diagnosis • Irritability • Full fontanel • Poor feeding • Elevated or subnormal temperature • Vomiting • Lethargy • Altered consciousness levels • Increased intracranial pressure (ICP) • Kernig’s & Brudzinski’s signs present 14. Herf C, et al, Meningococcal disease: recognition, treatment, and prevention, The Nurse Practitioner, 23:8, 1998, 33
Case Definitions Diagnosis • Confirmed case • isolation N. meningitidis from blood, CSF, petechiae or purpuric lesions, synovial fluid, pleural fluid, pericardial fluid • Presumptive case • Gram negative diplococci in any of above normally sterile fluids • Probable case • + antigen test for organism in blood or CSF with illness profile for meningococcal disease 3. American Academy of Pediatrics, Meningococcal disease prevention and control strategies for practice-based physicians, Pediatrics, 97:3, 1996, 405
Laboratory Findings Diagnosis • Meningococcemia • isolation of N. meningitidis15 • left shift leukocytosis14, 15 • leukopenia (overwhelming disease)14 • coagulopathy15 • metabolic acidosis14 • proteinuria14 • increased urine specific gravity14, 15 14. Herf C, et al, Meningococcal disease: recognition, treatment, and prevention, The Nurse Practitioner, 23:8, 1998, 34 15. Howe WB, Meningococcemia heading off a killer, The Physician and Sportsmedicine, 24:2, 1996, 2
Laboratory Findings Diagnosis • Meningitis - CSF • + for N. meningitidis • Normal in early or overwhelming infection • WBCs - >90% segmented neutrophils • > protein levels • < glucose levels (< 60 mg/dL) 14. Herf C, et al, Meningococcal disease: recognition, treatment, and prevention, The Nurse Practitioner, 23:8, 1998, 34
Definitions Treatment • Primary case - occurs in the absence of previously known close contact with another case • Secondary case - occurs among close contacts of a primary case > 24 hours after onset of illness in primary case • Coprimary case - two or more cases occur among group of close contacts with illness onsets separated by < 24 hours 6. CDC, Control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 15
Treatment - Primary Cases Treatment • Appropriate antibiotics • Penicillin G1,14 • Cefotaxime1 • Ceftriaxone1,14 • Chloramphenicol (for penicillin-resistant)14 1. Apicella MA, Chapter 189: Neisseria meningitidis. In: Principles and Practice of Infectious Diseases, 4th ed. Eds. Mandell GL, et al. Churchill Livingstone, New York, 1995, 1903 14. Herf C, et al, Meningococcal disease: recognition, treatment, and prevention, The Nurse Practitioner, 23:8, 1998, 36
Definitions Control • Close contacts - • household members • day care center contacts • persons directly exposed to the patient’s oral secretions (e.g. through mouth-to-mouth resuscitation or kissing) • Organization-based outbreak - • three or more confirmed or probable cases during period < 3 mos. in persons with common affiliation, but no close contact • primary disease attack rate of >10 cases/100,000 • includes schools, universities, correctional facilities 6. CDC, Control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 15
Definitions Control • Community-based outbreak - • three or more confirmed or probable cases during period < 3 months among residents in same area with no close contact and not sharing common affiliation • primary attack rate of >10 cases/100,000 • includes towns, cities, counties • Population at risk -group of persons, who, in addition to close contacts, are considered to be at increased risk for disease, when compared with historical patterns of disease risk in the same population 6. CDC, Control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 15, 16
Ten Steps to Control Control • Establish diagnosis • Administer chemoprophylaxis to contacts • Enhance surveillance, save isolates, review historical data • Investigate links between cases • Consider subtyping 6. CDC, Control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 20
Ten Steps to Control Control • Exclude secondary & co-primary cases • Determine if suspected outbreak is organization- or community-based • Define population at risk and determine size • Calculate attack rate • Select target group for vaccination • Refer to MMWR reference below for information 6. CDC, Control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 13-22
Chemoprophylaxis -Contact Cases Control • Rifampin • Ciprofloxacin • Ceftriaxone 4. CDC, Control and prevention of meningococcal disease and control and prevention of serogroup C meningococcal disease: evaluation and management of suspected outbreaks: recommendations of the Advisory Committee on Immunization Practices (ACIP), MMWR, 46:RR-5, 1997, 6
Menomune® - A/C/Y/W-135 Vaccination • Meningococcal Polysaccharide Vaccine, Groups A, C, Y and W-135 Combined16 • Dose 0.5 ml, subcutaneously16 • Protective antibody levels may be achieved 7 to 10 days post-vaccination16 • Revaccination may be indicated for persons remaining at high risk16 • Refractoriness to group C polysaccharide may limit secondary response24 16. Pasteur Mérieux Connaught Meningococcal Polysaccharide Vaccine Groups A, C, Y and W-135 Combined, Menomune ® - A/C/Y/W-135 package insert, June 1998, Copy serial 2494 24. Granoff DM, et al, Induction of immunologic refractoriness in adults by meningococcal C polysaccharide vaccination, J Infec Dis, 178:1998, 874
Indications Vaccination • Active immunization against serogroups A, C, Y, W-135 • May be used to prevent & control outbreaks of serogroup C • Does not protect against other serogroups or etiologic agents • Not for < 2 years of age except as short-term protection of infants >3 mos. against group A 16. Pasteur Mérieux Connaught Meningococcal Polysaccharide Vaccine Groups A, C, Y and W-135 Combined, Menomune ® - A/C/Y/W-135 package insert, June 1998, Copy serial 2494
Efficacy Vaccination • Group A & C - 85% to 100% in children > 4 yrs. & adults16 • Group A/C/Y/W-135 - 85% in 2 to 29 yr. olds in controlling group C outbreaks18 • Group A/C/Y/W-135 - 93% in preschoolers 2 to 5 yrs. in controlling group C outbreaks18 • Group A/C/Y/W-135 - > 4-fold increase increased bactericidal antibody; 90% subjects16 16. Pasteur Mérieux Connaught Meningococcal Polysaccharide Vaccine Groups A, C, Y and W-135 Combined, Menomune ® - A/C/Y/W-135 package insert, June 1998, Copy serial 2494 18. Rosenstein N, et al, Efficacy of meningococcal vaccine and barriers to vaccination, JAMA, 279:6, 1998, 435, 437
Vaccine Use Vaccination • Routine vaccination recommended for high risk groups: • deficiencies in late complement components (C3, C5-C9) • functional or actual asplenia • persons with laboratory or industrial exposure to N. meningitidis aerosols • travelers to, and residents of, hyperendemic areas such as sub-Saharan Africa 16. Pasteur Mérieux Connaught Meningococcal Polysaccharide Vaccine Groups A, C, Y and W-135 Combined, Menomune ® - A/C/Y/W-135 package insert, June 1998, Copy serial 2494
Vaccine Use Vaccination • Consider vaccination for • college students to reduce risk as recommended by the American College Health Association (ACHA)16 • household or institutional contacts16 16. Pasteur Mérieux Connaught Meningococcal Polysaccharide Vaccine Groups A, C, Y and W-135 Combined, Menomune ® - A/C/Y/W-135 package insert, June 1998, Copy serial 2494
Contraindications, Warnings Vaccination • Contraindications • defer during any acute illness • known sensitivity to thimerosal, or any other vaccine component • Warnings • contains latex rubber in stopper • expected response may not be obtained in immunosuppressed persons • do not give concurrently with whole-cell pertussis or whole-cell typhoid vaccines • As with any vaccine, vaccination does not protect 100% of all susceptible individuals 16. Pasteur Mérieux Connaught Meningococcal Polysaccharide Vaccine Groups A, C, Y and W-135 Combined, Menomune ® - A/C/Y/W-135 package insert, June 1998, Copy serial 2494
Precautions Vaccination • Precautions • health care worker to assure safe and effective use of vaccine • epinephrine (1:1000) to be immediately available • review patient’s history and current health • use separate, sterile syringe and needle for each patient • avoid intradermal, intramuscular, intravenous injections 16. Pasteur Mérieux Connaught Meningococcal Polysaccharide Vaccine Groups A, C, Y and W-135 Combined, Menomune ® - A/C/Y/W-135 package insert, June 1998, Copy serial 2494
Adverse Reactions Vaccination • Mild, consisting mainly of pain & redness at injection site for 1 to 2 days • Transient fever in < 2% of young children • No significant systemic reactions reported in 150 adults observed • Other reactions - mild to moderate headaches, malaise, mild chills and fever 16. Pasteur Mérieux Connaught Meningococcal Polysaccharide Vaccine Groups A, C, Y and W-135 Combined, Menomune ® - A/C/Y/W-135 package insert, June 1998, Copy serial 2494
New Developments PCR Testing • PCR (polymerase chain reaction) testing peripheral blood (buffy coat) used in research laboratories:19 • 100% specificity • rapid & sensitive • sensitivity unaffected by antibiotic treatment • serotype can be identified • May also be used on normally sterile fluids such as CSF 19. Newcombe J, et al, PCR of peripheral blood for diagnosis of meningococcal disease, Journal of Clinical Microbiology, 34:7, 1996, 1637
New Developments Treatments • Additional data required to establish efficacy of dexamethasone therapy to control inflammation20,21 • Rare, intermediate penicillin-resistant isolates in Europe, South Africa, North Carolina20 • Chloramphenicol-resistant serogroup B strains in Vietnam & France22 20. Quagliarello VJ, Scheld WM, Treatment of bacterial meningitis, N Engl J Med, 336:10, 1997, 710, 713 21. Schaad UB, et al, Steroid therapy for bacterial meningitis, Clin Infect Dis, 20, 1995, 689 22. Galimand M, et al, High-level Chloramphenicol resistance in Neisseria meningitidis. N Engl J Med,339:13, 1998, 868
New Developments Vaccines in Development • Conjugate vaccines • Single strain, outer membrane protein (OMP) vaccines • Recombinant multivalent serosubtype vaccines • Lipopolysaccharide (LPS) vaccines 10. Poolman JT, Development of a meningococcal vaccine, Infectious Agents and Disease, 4:1, 1995, 24