Download
1 / 77
770 likes | 1.02k Vues
Obesity: An Epidemic in America 15 Jul 2004. Kevin deWeber, MD, FAAFP Family Physician Primary Care Sports Medicine. Objectives. Review the scope and importance of obesity Know how to diagnose obesity and classify its severity based on comorbidity

E N D
Obesity: An Epidemic in America15 Jul 2004 Kevin deWeber, MD, FAAFP Family Physician Primary Care Sports Medicine
Objectives • Review the scope and importance of obesity • Know how to diagnose obesity and classify its severity based on comorbidity • Know know how to treat each severity class of obesity • Know how to prescribe behavioral modification, diet, exercise, medications and surgical treatments for obesity
Body Mass Index (BMI) is the global method of determining overweight/obesityBMI = wt/ht²(kg/m²)(lbs/in²)x704.5
Definitions • Normal: BMI 18 - 24.9 • Overweight: 25 -29.9 • Obese: >= 30 • Class I 30 - 34.9 • Class II 35 - 39.9 • Class III >= 40
Etiology of obesity • Too much food intake • Insufficient energy output • Not enough exercise • Low resting metabolic rate • Genetic predisposition • Environment favoring weight gain • Psychological stressors
Evidence review for etiologyPublic Health Nutr 2004 Feb;7(1A):123-46 • Convincing evidence as risk factors: • Sedentary lifestyle • High intake of energy-dense, micronutrient-poor foods • Probable risk factors: • Sugar-sweetened soft drinks and fruit juices • Adverse social and economic conditions
Hypertension Dyslipidemia Diabetes mellitus Coronary artery dz. Cerebrovascular dz. OVERALL MORTALITY HIGHER! Gallbladder dz. Sleep apnea Osteoarthritis Gout Cancers Colon Breast Prostate Uterus Cervix Obesity is associated with increased risk of co-morbid conditions:
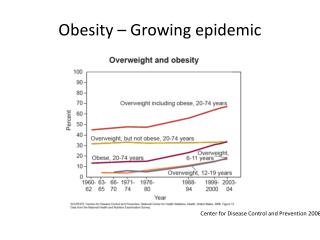
The scope of Obesity • Two thirds of American adults are overweight! • 31% are obese! • The prevalence is increasing! • Consumes 7% of national health care budget • HCP’s only counsel about 40% of obese patients
Goals of treatment • Get patients to look like models? • NOT • Get patients to their ideal body weight? • NOT practical usually • Get patients to lose 5-10% of body weight? • HOPEFULLY • Get patients to exercise and reduce their mortality risk? • DEFINITELY!
Set reasonable expectations • Gradually develop regular exercise • Gradually develop more healthy eating • Shoot for losing 5-10% of body weight first
Why the not-so-lofty goals? • Rarely do obese patient achieve IBW • Falling short leaves patients disappointed and highly susceptible to re-gain of lost weight • Health can be achieved WHILE still obese • “Healthy Obesity” concept
“Healthy Obesity” • Physically-fit obese patients have LOWER mortality rates than unfit normal-weight persons! • Being thin doesn’t guarantee being healthy • Being fat doesn’t HAVE to be unhealthy • Physical activity and cardiovascular fitness are much more predictive of health than body weight
Relative risk of all-cause mortality Obese UNfit Normal UNfit Obese FIT Normal FIT
Relative risk of cardiovascular disease Obese UNfit Normal UNfit Obese FIT Normal FIT
Despite the protection against cardiovascular dz. and all-cause mortality that cardio-respiratory fitness incurs, obesity still has its problems. • Osteoarthritis • Decreased quality of life • Social discrimination • Functional limitations
HIGH RISK Coronary artery dz Sleep apnea Type 2 diabetes RISK FACTORS Age (men>45, W>55) HTN LDL > 160 HDL < 35 Impaired fasting glucose FH of premature CAD Osteoarthritis Gallstones Stress incontinence Smoking Risk-stratifying obese patients
Choosing treatments • Determine BMI • Determine # of risk factors • Determine treatment options based on combination of the above
The single BEST method of treatment for obesityis... EXERCISE
Goals of treatment • Get patients to look like models? • NOT • Get patients to their ideal body weight? • NOT practical usually • Get patients to lose 5-10% of body weight? • HOPEFULLY • Get patients to exercise and reduce their mortality risk? • DEFINITELY!
Relative risk of all-cause mortality Obese UNfit Normal UNfit Obese FIT Normal FIT
Treating obesity demands a multi-faceted approach with chronic monitoring 1. Increased exercise 2. Decreased caloric intake 3. Behavioral modification 4. +/- Pharmacotherapy 5. +/- Surgery
Single vs. Combined Treatment • Diet alone: significant short-term weight loss, poor weight loss maintenance • Exercise alone: slight weight loss, good weight loss maintenance • Diet PLUS Exercise: more weight loss AND weight loss maintenance • Behavioral modification techniques are needed to increase diet/exercise effectiveness
1. Increased exercise • Exercise regularly • 150 minutes of moderate-intensity per week • 30 min 5 days a week • Start with brisk walking • Work up to 300 min a week • 60 min 5 days a week • Better weight loss maintenance
Facts on exercise in obesity tx. • Exercise alone only leads to slight wt loss but marked reduction in mortality • Aerobic exercise during wt loss lessens loss of FFM • Resistance exercise during wt loss preserves FFM and may help maintain wt loss • Any type of exercise helps maintain wt loss, but duration must be 300 minutes a week • Compliance may be better with multiple short-bout sessions
* How good is exercise alone for weight loss? • Not very effective • 11 studies • 5 found no change in weight w/ Exercise alone • 6 showed slight weight loss w/ Exercise alone • 1-2 kg
* What kind of exercise is best for obesity treatment? • Aerobic exercise is necessary • Resistance exercise alone does not lead to weight loss • Best approach may be a combination of aerobic AND resistance training • Preserves fat-free mass, strength, endurance • Maintains weight loss best
Kraemer WJ et al. Influence of exercise training on physiological and performance changes with weight loss in men. Med Sci Sports Exer 1999 Sep;31(9):1320-9.
* What is the effect of exercise intensity on weight loss? • Not much, as long as it is moderate to high • However, high-intensity aerobics leads to: • Better preservation of muscle mass • Greater LDL reduction • Better strength and endurance
Intermittent vs. continuous exercise for weight loss • Probably equal efficacy • Encourage use of Pedometers • Goal: 10,000 steps a day • Less for older pts, those w chronic dz • More for children
* What role does exercise have in weight loss maintenance? • A HUGE role • Best with 300 min/week
“Prevalence of leisure-time physical activity among overweight adults--United States, 1998.” • Two thirds of overweight persons trying to lose weight reported using physical activity as a strategy for wt loss • However, only 1/5 reported being active at recommended levels (30 min/day,most days). • MMWR 2000 Apr;49(15):326-30.
Counseling patients to increase exercise • Use the 5 A’s of counseling:\ • Address the agenda • Assess • Knowledge, beliefs, concerns, feelings, stage of change • Advise • Personalized exercise recommendations • Assist • Provide support, identify barriers and resources • Arrange follow-up
Tailor counseling to the patient’s stage of change • Pre-contemplation - not remotely interested • Contemplation - considering wt loss • Preparation - starting to make small changes • Action - meeting behavior change criteria • Maintenance - steady behavior over time
Example: Counseling a Pre-contemplator • Provide handout on health benefits of weight loss and exercise • Discuss barriers to exercise
Example: Counseling a patient in preparation phase • Give specific advice on Frequency, Intensity, Time and Type of exercise (FITT)
Specific Exercise Recommendations:FITT • Frequency: 3-5 days a week • Intensity: 55-90% of max heart rate • Time: 30-60 minutes • Gradually work up to this • Start with brisk walking 10 min • Work up to 60 min • Type: aerobic, resistance NHLBI, ACSM
Follow-up after initial counseling • See patient two weeks later and every month • Ask about progress • Encourage! • Ask about barriers • Discuss remedies • Weigh patient • Follow cholesterol, blood sugar, BP, etc.
2. Decreased caloric intake • 500 - 1000 kcal/day less than usual • Lose 1-2 lbs/week • Women: 1000 - 1200 kcal/day total diet • Men: 1200 - 1500 kcal/day total diet National Heart, Lung, and Blood Institute. Clinical guidelines on the identification, evaluation, and treatment of overweight and obesity in adults: the evidence report. 1998.
Step I DietA low-fat, low-calorie diet • Fat: <30% of total calories • Protein: about 15% of total calories • Carbohydrate: >55% of total calories • Cholesterol < 300 mg/day • Saturated Fatty Acids 8-10% of total cal • NaCl <6 gm • Fiber 20-30 gm
Step I Diet success • 8% wt loss over 6 months
What about Low-carb diets? • Range from 20-90 gm carbs/day • Atkins: start 20 gm/d, go up from there • Otherwise, eat what you want • Induces lipolysis & ketosis – minor side effects • 2003 meta-analysis: wt loss was a/w: • Longer diet duration • Restriction of calorie intake but not specifically carbs • No adverse efx on LDL, HDL, fasting glucose BP
5 RCT’s on low-carb vs low-fat diet in 2003/2004 • Low-carb diets show greater wt loss at 6 mos • 4-6% more body wt, or 4-5 more kg • One study 12 mos: no significant difference in wt loss • Low-carb showed better lipid profiles • Lower TG • Higher HDL • Same reduction in LDL • Same improvement in insulin sensitivity
How do low-carb diets work? • Am J Clin Nutr 2004 May;79(5):899S • Reviewed wt loss studies and examined calorie intake and expenditure • Wt loss was related to ENERGY BALANCE, not macronutrient type • CONCLUSION: Low-carb diets may influence satiety • Research needed
Zone Diet • 40% carbs, 30% protein, 30% fat calorie distribution • Promoted to reduce insulin:glucagon ratio leading to balanced eicosanoid ratio, leading to • reduced chronic dz, autoimmune dz, fatigue • enhanced wt gain, longevity, mental performance • Literature review: little scientific basis • J Am Coll Nutr 2003 Feb;22(1):9-17
South Beach Diet • No carbs for 2 weeks • Tho not a “low-carb” diet • Reintroduce only low-glycemic-index carbs • Certain fruits, veggies, whole grains • Heavy on healthy meats, esp. fish • No saturated fats; more healthy monounsaturated fats • Certain nuts, olive oil • Theoretically sound, but LACKS SCIENTIFIC CREDIBILITY
3. Behavioral Modification • Self-monitoring • Stimulus control • Body image and self-esteem counseling • Stress management • Social support
Self-monitoring • One of the MOST HELPFUL TOOLS IN OBESITY MANAGEMENT • Observation and recording of behaviors • Total calorie intake, fat grams consumed, food groups used, situations that promote overeating, amount/intensity of exercise, weight, body composition, etc. • Provides patient objective feedback so improvements can be made