Download
1 / 80
810 likes | 1.21k Vues
Positional Plagiocephaly The Shape of Affairs. November 21, 2009 Patricia Mortenson Dr. P. Steinbok Alan Keith. Agenda (Approximate). 1:00- 1:15 Definition, incidence, risk factors 1:15- 1:45 Synostosis differential (Dr. Steinbok ) 1:45 - 2:30 Assessment, treatment, outcomes,

E N D
Positional PlagiocephalyThe Shape of Affairs November 21, 2009 Patricia Mortenson Dr. P. Steinbok Alan Keith
Agenda (Approximate) • 1:00- 1:15 Definition, incidence, risk factors • 1:15- 1:45 Synostosis differential (Dr. Steinbok) • 1:45 - 2:30 Assessment, treatment, outcomes, sequelae • 15 minute stretch break • 2:45 - 3:15 Head banding (Alan Keith) • 3:15 - 3:30 Clinical pathways, future, resources • 3:30 - 4:00 Questions & problem solving
OBJECTIVES • Define positional plagiocephaly & risk factors • Be aware of differential diagnoses • Learn assessment techniques • Understand treatment guidelines • Describe outcomes & sequelae • Know how and when to make appropriate referrals in BC
PLAGIOCEPHALY? • “oblique head” • Causes • Deformational forces on moldable skull • Nature of the infant skull • Uterine & post-natal positioning • Gravitational forces • Correlation with torticollis
INCIDENCE • More cases with Back to Sleep (Persing et al., 2003) • At birth • 13% in singletons • Flat spots in 56% of twins (Peitsch et al., 2002) • 61% asymmetry of the head; 16% torticollis (Stelleagen et al., 2008)
Natural History • Followed 200 infants recruited at birth • Looked at plagiocephaly/brachycephaly: • 16% at 6 weeks • 19.7% at 4 months • 6.8% at 12 months • 3.3% at 24 months (Hutchison et al, 2004)
Boy First born Multiple birth Prematurity Intrauterine constraint Torticollis Developmental delay Macrocephaly Caregiving Factors Bottle feeding Tummy time < 3X/day Tummy time < 5 min/day Positioning in crib (van Vlimmeren et al., 2007; Hutchinson et al., 2003; Losee et al., 2007) RISK FACTORS
Plagiocephaly & Torticollis • Variable reported co-relations: e.g. • From 5 – 67% in Texas wide review of facilities/cases • Variation in diagnosis of CMT and SCM imbalance • Depends on specialty of facility/service Pivar & Scheuerle, 2006
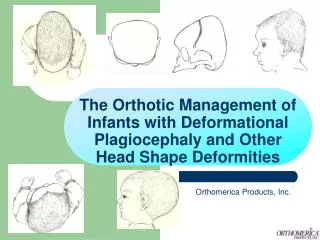
Occipital Positional Plagiocephaly www.plagiocephaly.org • Unilateral occipital flattening • Ear may be forward (Ipsilateral) • Forehead and cheek may be forward (Ipsilateral)
Brachycephaly www.plagiocephaly.org • Bilateral occipital flattening • Side of head widened
Positional Scaphocephaly www.plagiocephaly.org • Long and narrow head • More common in premature babies
HISTORY • Pregnancy, Birth & Neonatal history • When did parents first notice • Stayed same, gotten better/worse? • Torticollis? • What strategies have they already tried
HISTORY • Positioning for sleep, feeding, play • ? Tummy Time • Time spent in car seats, swings etc. • Development
CLINICAL ASSESSMENT • View from top, back, sides, front
CLINICAL ASSESSMENT • Describe shape of head
Eye symmetry & shape When in doubt refer to neurosurgery CLINICAL ASSESSMENT
Clinical Assessment • Check head turning and tilt • If possible, assess in sitting, supine & prone
Measurement • Challenges: • 2D measures on 3D object • Squirmy subjects • Variety of methods: • Visual ratings • Anthropometric (caliper measures) • Digital photos • CT scan • Laser scanner
Measurement Issues • Issues with • Classification • Reliability • Cost • Radiation & Sedation (Mortenson & Steinbok, 2006) • Need standardized classification system (McGarry et al., 2008)
For now…. • Argenta’s clinical classification • Severity assessment sheets available at: www.cranialtech.com • ? Reliability / validity
Argenta’s Classification • Type I just back of skull • Type II adds mal position of I/L ear • Type III adds forehead deformity • Type IV adds facial deformity • Type V adds temporal bossing or C/L bossing Argenta, 2004
Argenta’s Classification • Moderately reliable for Types I – IV (flatenning, ear malposition, frontal bossing, facial asymmetry) • but NOT for vertical skull height (Spermon et al, 2008) • ? Degree & responsiveness, ? Validity
Measurement - Brachycephaly • Cranial Index Maximum head breadth X 100 Maximum head length Scaphocephalic – up to 75.9 Brachycephalic – 81 and over • However ? New norms – wider head shapes with supine sleeping (Pomatto, et al., 2006)
Argenta’s Classification • Type I central posterior skull • Type II widening of the skull • Type III Temporal or vertical skull growth Argenta, 2004 • ? Reliability/validity
Rapid head growth Positioning for prevention and treatment Reverse process TREATMENT - Positioning
SLEEP POSITION • Place in crib so baby looks into room on the “round” side • Place mobile/crib mirror on “round” side • Turn head when asleep
SLEEP PRODUCTS • American Academy Position Statement “We recommend that firm flat bedding be used for normal healthy infants, with sheets and light blankets as needed, but without products to maintain the sleeping position.” www.cps.ca/english/statements/IP/cps98-01.htm#sleep
Safe T Sleep www.safetsleep.com Not approved by CPA Cautious use, Hutchison et al., 2007 POTENTIAL PRODUCTS
POTENTIAL PRODUCTS • Cranial cup • Custom molded “dish” for head to rest in during sleep • Weak evidence that effective in correcting early plagio (Rogers et al., 2008) • ? Safety and approval for use
UPRIGHT • Use of carriers • Hip belts & wide straps Ergo carrier Baby Trecker
PLAY POSITION • Awake & up • Tummy time • Supported sitting • Side lying for play
TUMMY TIME • Start with short but FREQUENT times • Options include: • On chest • Over legs • Supported on Floor
TUMMY TIME TEACHING BE: • Encouraging • Realistic • Demonstrate on baby OR doll
BUMBO Not all babies tolerate never use on an elevated surface supervise www.bumbosafety.com
SIDE LYING • On Round side • Best for pre-rollers • Rolled blankets • “Sleep” positioning devices
Bottle feed from “round” side Feed from “round” side in highchair FEEDING POSITION
BABY EQUIPMENT • Car seat stays in car • Stroller 101 • Limit Swing Use • Good equipment
IMPORTANT FACTORS • Multiple options for caregivers • Realistic • Demonstration as needed • Address any developmental factors
TREATMENT - Orthotic Headband • Indications • Moderate/severe • Face involved • Positioning not working • How it works • Wear • 23 hours/day for months • Limitations • Cost • Commitment • Hot weather
TREATMENT – Other issues • Torticollis – need to treat • Positioning not as effective(Losee et al., 2007) • Motor & Developmental delays • Parental guilt
OUTCOMES • Natural improvement (Hutchison et al., 2004) • Conflicting evidence – 3 systematic reviews • Positioning OR headband > than leaving be • Positioning = headband but takes longer • Helmet > positioning (most studies) (Bialocerkowski et al., 2005; McGarry, 2008; Xia et al., 2008)