Download
1 / 52
530 likes | 773 Vues
Oral Health Surveillance in the US & States. Mike Manz, DDS, MPH University of Michigan and ASTDD Consultant Texas Oral Health Summit: Advocacy, Equity & Access Austin, Texas September 9-10, 2004. Oral Health Surveillance – State of the States . Mike Manz, DDS, MPH

E N D
Oral Health Surveillance in the US & States Mike Manz, DDS, MPH University of Michigan and ASTDD Consultant Texas Oral Health Summit: Advocacy, Equity & Access Austin, Texas September 9-10, 2004
Oral Health Surveillance – State of the States Mike Manz, DDS, MPH University of Michigan and ASTDD Consultant
Great (Lake) State R e a l l y G r e a t T o w n # N W E 2 0 0 0 2 0 0 4 0 0 M i l e s S
Surveillance My definition: What you want to know about who(m?) and what you do with it.
Surveillance Defined • Surveillance vs. Surveys vs. Screening • Surveillance in public health is “the ongoing systematic collection, analysis and interpretation of outcome-specific data for use in the planning, implementation and evaluation of public health practice.” Thacker SB, Berkelman RL. Public health surveillance in the United States. Epidemiol Rev 1988;10:164-90.
Specific Oral Health Surveillance Aims • Address problems described in Report of the Surgeon General on Oral Health at state (Texas) level www.surgeongeneral.gov/library/oralhealth/ • And… A National Call to Action to Promote Oral Health www.nidcr.nih.gov/sgr/CallToAction.asp • Assess progress toward Healthy People 2010 objectives (HHS- Office of Disease Prevention and Health Promotion) www.healthypeople.gov
Report of the Surgeon General on Oral Health • Purpose of reports: “frame the science on vital health issues in a way that have helped educate, motivate and mobilize the public to more effectively deal with those issues” • Emphasized racial and socio-economic disparities particularly in children
HP 2010 - Oral Health • Goal : Prevent and control oral and craniofacial diseases, conditions, and injuries and improve access to related services. • Objectives: 17, including oral health status, individual and population preventive exposure, and access to care • Age groups: • Caries: 2-4, 6-8, 15, adults • Sealants: 8, 14 • Edentulism: 65-74 • Periodontal Disease: 35-44 • Oral Cancer Screening: ge 40
Existing Data Sources • National Level • NCHS - NHANES, NHIS • Fluoridation Census • NIDCR • State Level • BRFSS • WFRS/ MWF • YRBS • PRAMS • Previous surveys • Medicaid and private insurance data (claims - no dx codes)
Existing Data Sources • NIDCR/CDC Data Resource Center • Existing national survey data and OH related questions
Existing Oral Data - BRFSS • Core component • Optional modules and • State added questions addressing: • Access to care/last dental visit • Teeth cleaning/oral hygiene • Dental insurance • Edentulism/missing teeth • Tobacco use
Collecting New Data (Filling Gaps) • Questionnaires vs. in-mouth screening • Conditions assessed • Resources • Costs • Response • Who’s doing the assessing • Self Assessment Reliability (pending)
ASTDD www.astdd.org • State Activities • Best Practices • Resources Links including state oral health programs • Publications • Basic Screening Survey (BSS) • Seven Step Model • Program Guidelines • Technical Assistance
Best Practice Approaches – State Oral Health Surveillance • Characteristics/utility of a good system • Sources of data • Building an OH surveillance system • National Oral Health Surveillance System (NOHSS) as a basis • Using existing data and integrating with existing systems (YRBS, PRAMS, BRFSS) • In-mouth surveys as needed
Best Practice Approaches – State Oral Health Surveillance • Emphasis on • defining resources • use of system data for planning/decision making • importance of dissemination and partnering • CDC model cited: resources > activities > outcomes www.cdc.gov/oralhealth/library/infrastructure.htm
Best Practice Approaches – State Oral Health Surveillance • Oral health surveillance system evaluation criteria • Impact/effectiveness – important indicators and dissemination • Efficiency – regular schedule, cost effective data collection, analysis, and dissemination • Sustainability – continuous over years to analyze trends • Collaboration/integration • Resources and partnering • Integrating oral health into other programs • Objectives/rationale – clear on why system exists and how data will be used
Guidelines for State and Territorial Oral Health Programs • Based on 1988 IOM Future of Public Health Report model with components: • Assessment • Policy development • Assurance
Guidelines for State and Territorial Oral Health Programs • Specific guidelines on Assessment • Oral Health Status and Needs • Monitor oral health status and needs • Assess oral health in special populations • Document dental service needs • Analyze determinants of oral health (includes assessment of OH services, workforce, and knowledge/perceptions of constituents and care providers) • Assess state and local fluoridation
Guidelines for State and Territorial Oral Health Programs • Implement OH surveillance system • Develop (Seven Step Model) • Maintain – systematic continuous collection • Disseminate findings • Support local surveillance • Surveillance (evaluation) of OH programs/services • Integrate with other state systems • Coordinate/collaborate with other government/industry/university etc. surveillance • Surveillance of potential OH hazards (radiation, amalgam (Hg), infection control, nitrous oxide…)
ASTDD Resources • Seven Step Model • Basic Screening Survey (BSS) • BSS EpiInfo program module
Seven Step Model • Lays out the steps in developing a needs assessment system (simple to complex) • Identify partners – form advisory committee • Conduct a self assessment • Plan the needs assessment • Collect data • Organize and analyze data • Prioritize issues and report findings • Evaluate the needs assessment
Objectives of BSS Surveys • To provide information not available from existing data sources • Assess basic (but important) indicators - simple training for non-dental professionals • To provide information on: • Caries experience and untreated caries • Dental sealants • Can add - dental trauma, malocclusion, dental fluorosis, oral pathology, missing teeth…..
Objective Objectives • Derive population estimates from sample • Get good estimates - representative sample • Be able to estimate statistically how good these estimates are (probability sampling) • Avoid biases in sample (good design and following protocol) • Avoid biases in data collection (standardization and following protocol)
What You Can Get • State estimates • County specific estimates for bigger counties • Estimates by SES (F/R lunch) • Estimates by urban/rural • Estimates by health region
What You Can Do With It • Compare to national (NHANES) and other state (NOHSS) data / report (NOHSS, MCH) • Track disease trends over time/ assess progress toward Healthy People Objectives • Explore variations by geography, SES, etc. = disparities • Provide for optimal program planning for improving the oral health of the population
What’s going on? - CDC • Data Systems • MWF• NOHSS • Oral Health Maps• Synopses • WFRS
National Oral Health Surveillance Systemwww.cdc.gov/nohss/ • CDC/ASTDD – monitor disease burden • 8 oral health indicators • Dental visits (NHIS, BRFSS) • Teeth cleaning (BRFSS) • Edentulism (BRFSS) • Fluoridation (WFRS) • Caries experience (BSS) • Untreated caries (BSS) • Dental sealants (BSS) • Oral cancer (Vital statistics, cancer registries)
National Oral Health Surveillance System • Inclusion Criteria for Caries/Sealants Data • Within past 10 years • Statewide probability sample • Trained/calibrated examiners (yearly) • NIDCR or BSS criteria used • SUGGEST minimally 3rd grade (K-2) • Stratified by grade (vs. age) • Submitted by school year • Would like nonresponse adjustment • % F/R lunch for sample kids, schools, and state
Examples - Pennsylvania • Battery of Surveys 1998-2000 • School – Grades 1,3,9 and 11 (caries counts) • Parent interview on subset (SES, insurance, perceived need, concerns, parents oral history, dental knowledge) • School nurses – log of emergency visits/dental • Fluoridation census • State mandated oral screenings - entry (K or 1), 3, and 7 - school summaries dmf and treatment need (since 1949 - boxed in Harrisburg) = untapped resource
Illinois • Just completing BSS survey / Division of Chronic Disease (CV and obesity) BMI • 1994 DMF survey with trauma/mouthguards info • BRFSS, cancer registry, PRAMS, NOSHA, MCH, Medicaid - summary of data collected/how/ and when, Illinois specific indicators • Communication and information to collect on regular basis from local agencies (may develop ground-up surveillance system) • Workforce survey (practice characteristics, retirement) • Fluoride survey – awareness of dentists/hygienists
Kentucky • LARGE statewide surveys in 1987, 2001 • Presently developing surveillance system • 3 year cycles of replicate samples conducted annually • State representation annually, county level after 3 years and annual surveys merged for improved state estimates
Ohio • Large surveys – 87, 92-93, 98-99, 04-05 • State to county level surveys (vs. VT) • Down to grade 3 and BSS indicators • County profiles website • Detailed data available to counties for monitoring, and reporting, and grant applications $$$$$
Ohio cont. • Annual data • 25 sentinel sites (reassessed) • MCH requirements • Need/Readiness assessment • Hospital data (OH Hospital Assn) • Workforce data • Census data • Medicaid Data • Ohio Family Health Survey
Summary • Oral Health Surveillance: Past, Present, and Future Challenges. J Public Health Dent 2003;63(3):141-9. • Trend to state and local data collection • Integration with existing systems • Visual only simpler oral indicators • Variety of conditions/behaviors (vs. DMF) • Timely analysis and dissemination
Summary – Logical Conclusion The better you can define the problem, the better your chances of obtaining resources and addressing the problem.
Bonus Time - Sampling Issues • Representative of Who? • Precision of population estimates • Level of Estimates • State • Region • County • (Small Area Estimation) • Subpopulations of interest
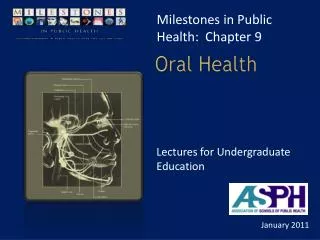
Methods • Representative PPS (probability proportional to size) sampling of schools to produce state and subpopulation estimates • Systematic Selection from an ordered list to achieve “implicit stratification” on region, urban/rural, and free/reduced lunch eligibility, …. your choice
# S o # S o u t h w e s t e r n D i s t r i c t N o r t h C e n t r a l D i s t r i c t N o r t h w e s t e r n D i s t r i c t Sampled School Districts and Regions Pittsburgh Philadelphia
P o p u l a t i o n b y C o u n t y 4 5 0 0 - 1 0 0 0 0 0 P I T T S B U R G H S D 1 0 0 0 0 P H I L A D E L P H I A C I T Y S D Sampled School Districts and County Populations P A O H N A S c h o o l D i s t r i c t s 1 - 2 5 0 0 0 0 2 5 0 0 0 1 - 4 5 0 0 0 0 4 5 0 0 0 1 - 7 0 0 0 0 0 7 0 0 0 0 1 - 1 5 0 0 0 0 0 N W E 1 0 0 0 1 0 0 2 0 0 M i l e s S
Sampling Terms • Probability Sampling • Purposive (“Expert Choice”) Sampling • Simple Random Sampling • Cluster Sampling • Stratification and Stratified Random Sampling • Systematic Sampling (Implicit Stratification) • Probability Proportional to Size (PPS) • Weights • Oversampling • Nonresponse (BAD)
But how many kids should we screen??????? • Simple but unsatisfying answer – how many can you screen? • Certain % of the population? - nope • Real first question - how much precision do you want (or will settle for) at what level? • Second question – do you have other data for sample size calculation • Third question – what’s your sample design?
Sample Size –Effects of Sample Design • Stratification – small gains in precision • Clustering – potentially big loss in precision • Main variable(s) of interest • Design Effect – practical definition • Expected Non-response
Sample Size –Effects of Sample Design • In our case (BSS) – proportions • Simpler formula than continuous variables: • v(p0) = (1-f) p0 q0 / n-1 • Conservatively use p0 = 50% • For 95% CI = +/- 10% n = 97 • For 95% CI = +/- 5% n = 384 • For 95% CI = +/- 3% n = 1,066
Sample Size –Effects of Sample Design • Then multiply by estimated design effect • Remember basically the same calculations are appropriate for the designated population level, e.g. • If want this precision for regional level estimates and have 5 regions, then X 5 • If want this precision for county level estimates and have 35 counties, then X 35