Download
1 / 43
470 likes | 650 Vues
Immunology of endocrine diseases Aetiology BS936 autoimmunity component Professor Nelson Fernández.

E N D
Immunology of endocrine diseases Aetiology BS936 autoimmunity component Professor Nelson Fernández
There are over 80 types of autoimmune diseases. Many have overlapping symptoms. The most commonly cited complaints amongst autoimmune disease sufferers are fatigue, low-grade fever and sore muscles. Autoimmune diseases can affect any part of the body, including the nerves, muscles, endocrine system and digestive system.
Autoimmune disease results from a breakdown in immunological • tolerance
Mechanisms hypothesized to be involved in the breakdown of tolerance Failure to delete autoreactive lymphocytes Central tolerance failure Peripheral tolerance failure Molecular mimicry Abnormal presentation of self antigens Aberrant expression of major histocompatibility complex class II molecules Coupling of self and nonself antigens Overproduction of self antigens Disclosure of cryptic T-cell epitopes Release of sequestered self antigens Epitope spreading Polyclonal lymphocyte activation
Central tolerance = thymic education
Anti-CD20 therapy and B cells in autoimmunity. B cell depletion: a novel therapy for autoimmune diabetes? Hélène Bour-Jordan, Jeffrey A. Bluestone J Clin Invest. 2007;117(12):3642–3645
Autoreactive B cells play a role in autoimmune diseases by production of circulating autoantibodies and/or their role as antigen-presenting cells for autoreactive T cells after the capture of self antigens by cell surface autoantibodies that increase their antigen-presentation capabilities Rituximab and other anti-CD20 mAbs cross-link CD20 on the surface of B cells and induce B cell depletion mainly through ADCC, although complement-dependent cytotoxicity (CDC) and apoptosis have also been implicated. Anti-CD20–mediated B cell depletion prevents interaction with autoreactive T cells and reduces the amount of circulating autoantibodies, although with much slower kinetics.
Autoimmune endocrine diseases Thyroid Hashimoto’s disease (autoantibodies against thyroid peroxidase) Primary myxoedema (atrophy of the thyroid) Graves’ disease (autoantibodies against TSH-R) Pancreas Type I diabetes Adrenal Addison’s disease (chronic endocrine disorder; adrenal glands produce insufficient steroid hormones Gonads Autoimmune oophoritis (inflammation of the ovaries) Autoimmune orchitis (testicular pain involving swelling, inflammation and infection) Pituitary Lymphocytic hypophysitis (low production of one or more hormones by the pituitary gland due to autoantibodies and autoimmunity)
Aetiology of autoimmune disease • Genes • Environment
Thyroid autoimmunity Hypothyroidism Hashimoto’s disease Atrophic thyroiditis Hyperthyroidism Graves’ disease
AUTOIMMUNE THYROID DISEASES – GENETICS 22% concordance in monozygotic twins Susceptibility genes include: HLA-DR3 and/or -DR4. CTLA-4 polymorphisms
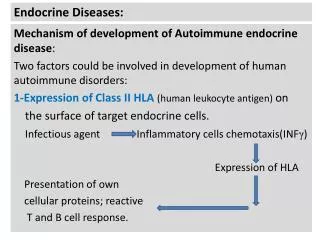
Nature of the associations: The MHC class II HLA-DR gene products present antigenic peptides to CD4+ helper T-cells. The polymorphic variants may present different autoantigenic peptides. CTLA-4 is a surface molecule on T-cells which binds CD80 and CD86 on antigen-presenting cells. Unlike CD28 on the T-cell, which activates the T-cells when it binds CD80 and CD86, CTLA-4 switches off the T-cell. The polymorphisms may therefore influence T-cell activation/inactivation.
AUTOIMMUNE THYROID DISEASES - ENVIRONMENTAL AND ENDOGENOUS FACTORS Female: Male ratio 5:1. At least partly due to modulation of the autoimmune response by oestrogens. Thyroid autoimmunity usually subsides during pregnancy, and rebounds post-partum. Stress. Bereavement, divorce, job loss may proceed onset. Neuroendocrine pathways affecting the immune system? Smoking: Weakly associated with Graves’ disease and strongly associated with development of opthalmopathy. Iodine: In areas of iodine deficiency, iodine supplementation associated with Graves’ disease.
TYPE I DIABETES – GENETICS Susceptibility genes include: HLA-DQ8 Resistance genes include: HLA-DQ6
TYPE I DIABETES – ENVIRONMENT INFECTION Coxsackie virus??? Echovirus??? DIET Wheat protein???
Incidence of spontaneous diabetes in geographically dispersed colonies of NOD mice at 20 weeks of age
Addison’s disease Deficient production of adrenocortical hormone Weakness, anorexia, nausea, vomiting, weight loss, hypotension
ADDISON’S DISEASE – GENETICS Female:Male ratio 4:1 Susceptibility genes: HLA-DR3 and/or DR4
Rheumatoid arthritis particularly affects the small joints of the hands and feet
Typical rheumatoid joint deformities in the hands. There is wasting of the small muscles of the hand, swelling of the metacarpophalangeal joints and a small subcutaneous nodule on the little finger. The fingernail ‘clubbing’ is characteristic of the pulmonary fibrosis from which this patient also suffered.
The knuckle joint shown here is inflamed and swollen, and the range of movement and strength of the joint are greatly reduced compared with a healthy joint
The disease process starts with inflammation of the lining of the joint -the synovium- and is followed by destruction of the underlying cartilage, and then the bone itself.
PATHOGENESIS http://fds.oup.com/www.oup.co.uk/pdf/0-19-262922-0c.pdf From Dr J. Martinez
TYPE III: IMMUNE COMPLEX DISEASE Rheumatoid Factor (RF) ~80% of patients. RF = “IgM anti-IgG antibody” TYPE IV: T-CELL MEDIATED DISEASE RA synovial fluid is enriched with macrophages, neutrophils, Tlymphocytes & dendritic cells. …PATHOGENESIS From Dr J. Martinez www.bio.davidson.edu/courses/immunology/Students/spring2006/Dresser/RA.html
…PATHOGENESIS T-CELL MEDIATED DISEASE en.sanofi-aventis.com/.../im/p_im_arthritis.asp From Dr J. Martinez
…PATHOGENESIS From Dr J. Martinez http://fds.oup.com/www.oup.co.uk/pdf/0-19-262922-0c.pdf
Normal synovial membrane: Film of 1-2 cells Type A and Type B cells RA synovial membrane: Several cell layers (2-10) Type A cells > Type B cells Subintima – angiogenesis and infiltration by mononuclear cells …PATHOGENESIS http://fds.oup.com/www.oup.co.uk/pdf/0-19-262922-0c.pdf From Dr J. Martinez
Onset: Insidious Main symptoms: Pain Stiffness – on waking and following inactivity Other symptoms: Fatigue and lethargy Low-grade fever Weight loss Progressive decline in physical function. CLINICAL FEATURES • From Dr J. Martinez
SUMMARY In the endocrine autoimmune diseases it is thought that, in genetically susceptible individuals, environmental factors lead to a breakdown in immunological tolerance. The actual environmental factors involved are unknown. Ref.: Most material from P. Delves (in Roitt and Delves, Essential Immunology, 10th Edition Blackwell)