Download

1 / 30
340 likes | 1.47k Vues
Understand core anatomy, muscle physiology, and the impact of low back pain on core stability. Learn about the benefits of lumbar stabilization exercises for pain relief and improved spinal health.

E N D
Physical Therapy Approachto Low Back Pain - Lumbar Stabilization Stacey Franz, DO, MSPT Medical Director, NorthEast Spine & Sports Medicine
Disclosures • I have no relevant financial disclosures
How our core supplies stability • Promote muscle stiffness to control segmental translation • segmental stability is dependent on recruitment of the deep local stability muscles • Anticipatory recruitment prior to functional loading provides protective stiffness • Proximal stability for movement of extremities • Generates force to control, limit range of motion • Concentric action through the range of motion • isometric action to hold position • Eccentrically control the return
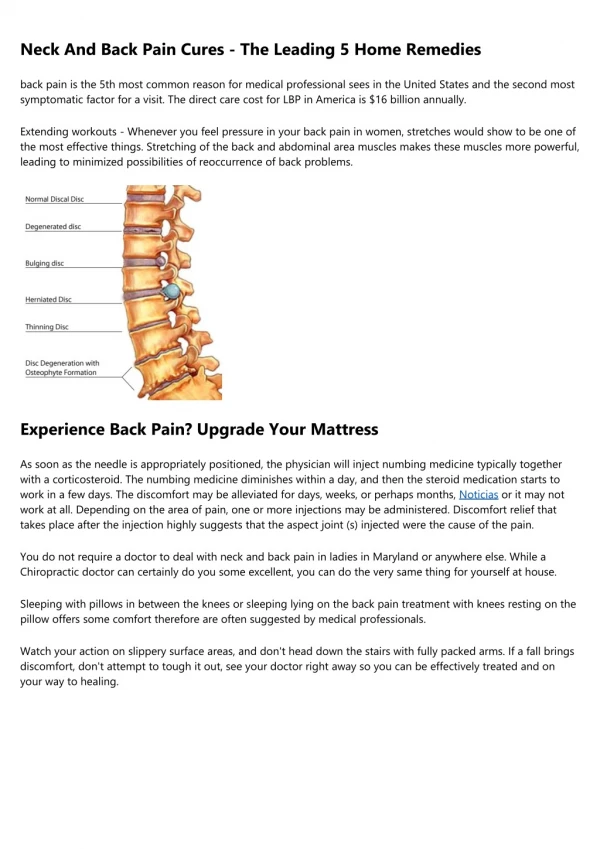
Anatomy of the Core – Lumbar Muscles • Muscles • Transversospinalis group • Rotatores, Interspinales, Intertransversarii, Multifidi • Erector spinae • Iliocostalis, Longissimus, Spinalis • Latissmusdorsi • Quadratuslumborus • Physiology • Poor mechanical contribution to movement production • Primarily Type I fibers = segmental stabilization • Optimal for proprioceptive feedback *Multifidi most important muscle in this group*
Anatomy of the Core – Abdominal Muscles • Muscles • Transversus abdominus • External obliques • Internal obliques • Physiology • Provide sagittal, frontal & transverse plane stabilization • Transversus abdominus • increases intra-abdominal pressure = dynamic stab. against rotational, translational stress • Necessary for anticipatory control • Activates prior to movement of the limbs or trunk to increase stability of the spine, prevent unwanted trunk movement • Activity contributes to spinal control • Attach to thoracolumbar fascia = add tension w/ contraction Cresswell 1994, Cresswell 1992, Hodges 1999
Anatomy of the Core – Hip Muscles • Muscles • Psoas • Glut medius • Glut maximus • Hamstrings • Physiology • Psoas tightness can be problematic • can lead to reciprocal inhibition of glut maximus, multifidus, erector spinae, internal oblique, TA • lead to Extensor mechanism dysfunction • increase shear and compressive forces at L4-L5 junction
Anatomy of the Core – Hip Muscles (continued) • Physiology • Glut medius weakness • increase frontal and transversus plane stress at patella-femoral joint and tibiofemoraljoint • synergistic dominance of TFL & quadratus lumborum • Glut maximus • Decreased activity can lead to pelvic instability, decreased neuromuscular control
What happens to the core when we have low back pain? • Inefficient muscular stabilization • Pain leads to inhibition of muscle control • Motor control deficit associated with delayed timing or recruitment deficiency • Transversus abdominus shows decreased ability to contract in patients with recurrent low back pain • Impairs our anticipatory control • Impairs our spinal control Stokes & Young 1984, Hides et al. 1994, Hodges & Richardson 1996, Hodges 1997, Ferreira 2004, Cresswell 1992, Hodges 1999
What happens to the core when we have low back pain? (continued) • Weakness and muscle fatigue • Multifidi atrophy in patients with chronic LBP • In unilateral acute/ subacute LBP, there is 31% side to side difference with atrophy of affected side - 3% in controls • Decreased endurance of extensors • Abnormal flexor to extensor strength ratios • Decrease in muscle integrity results in lack of control of segmental translation Richardson 1999, Jorgensen 1987, Ebenbichler 2001, McGill 2002, Siolie2001
What happens to the core when we have low back pain? (continued) • Decreased spine proprioception • Multifidi atrophy in those with LBP • Proprioception partly from multifidi • Difficulty repositioning into neutral spine posture • Loss of control of neutral joint position • Postural control shown to be altered in patients with chronic LBP • Single leg stance balance • Postural stability tests • Unexpected balance challenges • Trunk perturbation Bogduk1997, Hides 2004, O’Sullivan 2003, Ebenbichler 2001, Mok 2004, Wilder 1996
How Does Core Stabilization help Low Back Pain • Multifidi activation improves pain in acute & chronic LBP • Multifidi dysfunction does not correct automatically when pain resolves but specific training can correct dysfunction • Segmental stabilization training with co-contraction of Transversus abdominus and Multifidi • Abdominal bracing training stiffens the spine and improves stability • Exercise, in general, beneficial for low back • Slows degenerative conditions • Enhances nutritional benefits to spine Hides 1996, O’Sullivan 1997, Grenier 2007
Lumbar Stabilization Concepts • What does it entail: • Recruitment of proximal trunk & girdle muscles • Ability of agonists, antagonists, synergists, to work efficiently & interdependently • Facilitates balanced muscular functioning of the entire kinetic chain • How does it translate functionally: • Enhances neuromuscular control/ efficiency throughout the kinetic chain • Optimizes postural alignment & dynamic postural control • Affect arthrokinematics around lumbo-pelvic-hip complex • Promote dynamic strength
Lumbar Stab. Concepts (continued) • Neutral vs. Dynamic Stabilization • “Neutral spine stabilization” introduced in 1980s • Position of comfort where muscular support reduces stress on painful structures • “Dynamic stabilization” introduced in 1990s • more functional; multi-planar requiring acceleration & stabilization • interest increased after Joe Montana returns to football after lumbar spine surgery
Assessment of the Core • Prone instability test • Prone extension endurance test • Side bridge endurance test (quadratus lumborum endurance strength) • Straight leg raise • Pelvic bridging • Leg lowering test (lower abdominal strength) • Trunk curl • Hip external rotation strength • Modified Trendelenburg test (single leg squat with observation in frontal plane) • Single leg squat in sagittal plane • Single leg squat in transverse plane Akuthota et al 2008, Hicks 2005
Program Prescription • Be mindful of pain generators • Flexion vs. Extension vs. Neutral program • Exercises that span the spectrum of muscle contraction • Concentric (force production) • Eccentric (force reduction) • Isometric (dynamic stabilization) • Exercises that span body positioning • Supine • Prone • Quadruped • Sitting
Program Prescription (continued) • Progression should include additional reps rather than increasing duration of hold • Can perform 30 reps with 8 sec hold • Should challenge the patient by progression through function continuum • Slow to fast • Simple to complex • Low force to high force • Eyes open to eyes closed • Static to dynamic • Quality, not Quantity • Poor technique and neuromuscular control results in poor motor patterns & stabilization Akuthota 2008
Level 1- Stabilization Pelvic tilts • Supine • Diaphragmatic breathing • Abdominal bracing • Pelvic tilts • Arm lift • Leg lifts • Opposite arm lift/ leg lift • Marching • Bridging • w/ arms at sides • w/ arms at 90 degrees • w/ marching Bridging (http://www.netfit.co.uk)
Level 1– Stabilization (continued) Opposite arm/ leg (http://priorityhealthchiropractic.com) • Prone • Finding neutral • Glut sets • Arm lift • Leg extension • Opposite arm lift/ leg lift • Quadruped • Cat camel to find neutral • Rocking to find neutral forward/ backward • Single arm raise • Single leg extension • Opposite arm raise/ leg extension • Kneeling • Finding neutral
Level 1– Stabilization (continued) • Sitting • Finding neutral • Single arm lift • Single leg extension • Marching • Opposite arm/ leg lift (leg extended) • Opposite arm/ leg lift (marching) • Standing • finding neutral • Wall slide Wall slides
Level 2 – Stabilization Bridging w/ leg extension (www.arthritis.org) • Supine • Partial, diagonal curls • Single leg lowering • Opposite arm/ leg lowering • Bridging with leg extension • Bridging with one leg • Prone • Push ups against wall • Push ups with feet farther apart • Push ups on chair • Push ups on floor
Level 2 – Stabilization (continued) • Quadruped • Alternate arm/ leg with cuff weights • One arm reach • Kneeling • Rock with arms and weights overhead • With side kicks • P ush-pull with sticks • Lifting up and down • Half kneeling to standing • Sitting • Leg lifts • Opposite arm/ leg lift Kneel w/ side kick (http://www.studiopilates.com)
Level 2 – Stabilization (continued) • Standing • Hip flexion with weight cuffs • Double arm overhead with weight cuffs • Lunges • Push-pull with sick (up and down) • Ball pass vs light medicine ball use http://www.ironedge.com.au/
Level 3 – Stabilization • Supine • Double leg lowering with 5 lb cuff weight • Dead bug with arm/ leg cuff weights • Bridging with calves on ball/ upper back • Bridging with feet on ball • Prone • 2 Arms with 1 leg together • Trunk extension • Standing • Push/ pull with sticks www.ilovefitness.com
Additional Exercise • Level 4 • Sport-specific training • Pilates • effective option for core stabilization • Individuals performing pilates had better lumbo-pelvic control of the transversus abdominus than those who perform regular abdominal exercises or no abdominal exercises Herrington 2003
Summary of Citations • Akuthota V, Ferriero TM, Fredericson M. Core stability exercise principles. Curr Sports Med. 2008;7(1): 39-44. • BogdukN: Clinical Anatomy of the Lumbar Spine and Sacrum. Edinburgh, Churchill Livingstone, 1997 • Carman DJ, Blanton PL, Biggs NL. Electromyographic study of the anterolateral abdominal musculature utilising indwelling electrodes. American Journal of Physical Medicine 1972;51(3):113–29. • CresswellAG, Grundstrom H, Thorstensson A. Observations on intraabdominal pressure and patterns ofabdominal intra-muscular activity in man. ActaPhysiologicaScandinavica 1992;144(4): 409–18. • CresswellAG, Oddsson L, Thorstensson A: The influence of sudden perturbations on trunk muscle activity and intraabdominal pressure while standing. Exp Brain Res 1994;98: 336–341 • EbenbichlerGR, Oddsson LI, Kollmitzer J, et al: Sensorymotor control of the lower back: Implications for rehabilitation. Med Sci Sports Exerc2001;33:1889–98
Summary of Citations (continued) • Ferreira PH, Ferreira ML, Hodges PW: Changes in recruitment of the abdominal muscles in people with low back pain: Ultrasound measurement of muscle activity. Spine 2004;29:2560–6 • Flint MM, Gudgell J. Electromyographic study ofabdominal muscular activity during exercise. The Research Quarterly 1965;36(1): 29–37. • GrenierSG, McGill SM. Quantification of lumbar stability by using 2 different abdominal activation strategies. Arch Phys Med Rehabil. 2007 Jan; 88(1): 54-62 • Herrington L, Davies R. The influence of Pilates training on the ability to contract the Transversus Abdominis muscle in asymptomatic individuals. Abstract. 2003 • Hicks GE, Fritz JM, Delitto A, McGill SM. Preliminary development of a clinical prediction rule for determining which patients with low back pain will respond to a stabilization exercise program. Arch Phys Med Rehabil2005; 86:1753-62. • Hides J: Paraspinal mechanism and support of the lumbar spine, in: Richardson C (ed): Therapeutic Exercise for Lumbopelvic Stabilization, ed 2. Edinburgh, Churchill Livingstone, 2004, pp 59–74
Summary of Citations (continued) • Hides JA, Richardson CA, Jull GA: Multifidus muscle recovery is not automatic after resolution of acute, first-episode low back pain. Spine 1996;21:2763–9 • Hodges PW, Cresswell A, Thorstensson A. Preparatory trunk motion accompanies rapid upper limb movement. Experimental Brain Research 1999;124(1):69–79. • Hodges PW, Richardson CA, Jull GA. Evaluation of the relationship between laboratory and clinical tests of transversusabdominis function. Physiotherapy Research International 1996a;1(1): 30–40. • Hodges PW, Richardson CA: Contraction of the abdominal muscles associated with movement of the lower limb. Phys Ther 1997;77:132–42; discussion, 142–34 • Hodges PW, Richardson CA. Inefficient muscular stabilization ofthe lumbar spine associated with low back pain. A motor control evaluation of transversus abdominis. Spine 1996b;21(22): 2640–50. • Jorgensen K, Nicolaisen T: Trunk extensor endurance: Determination and relation to low-back trouble. Ergonomics 1987;30:259
Summary of Citations (continued) • Kennedy B. An Australian programme for management of back problems. Physiotherapy 1980;66(4):108–11. • McGill S: Normal and injury mechanics of the lumbar spine, in: Low Back Disorders: Evidence-Based Prevention and Rehabilitation. Champaign, IL, Human Kinetics, 2002, pp 87–136 • Mok NW, Brauer SG, Hodges PW: Hip strategy for balance control in quiet standing is reduced in people with low back pain. Spine 2004;29:E107–12 ----Bilateral standing on short base with eyes closed – LBP failed 4 times more than controls • O’Sullivan PB, Burnett A, Floyd AN, et al: Lumbar repositioning deficit in a specific low back pain population. Spine 2003;28:1074–9 • Richardson C, Jull G, Hodges P, et al: Traditional views of the function of the muscles of the local stabilizing system of the spine, in: Therapeutic Exercise for Spinal Segmental Stabilization in Low Back Pain: Scientific Basis and Clinical Approach. Edinburgh, Churchill Livingstone, 1999, pp 21–40
Summary of Citations (continued) • Richardson CA, Jull GA, Hodges PW, Hides JA. Therapeutic exercise for spinal segemental stabilization in low back pain. Scientific basis and clinical approache. Ediburgh: Churchill Livingston 1999 • SjolieAN, Ljunggren AE: The significance of high lumbar mobility and low lumbar strength for current and future low back pain in adolescents. Spine 2001;26:2629–36 • Urquhart DM et al. Manual Therapy 10(2005) 144-153 • Vezina MJ, Hubley-Kozey CL, Egan DA. A review of the muscle activation patterns associated with the pelvic tilt exercise used in the treatment of low back pain. The Journal of Manual and Manipulative Therapy 1998;6(4):191–201. • VezinaMJ, Hubley-Kozey CL. Muscle activation in therapeutic exercises to improve trunk stability. Archives of Physical Medicine and Rehabilitation 2000;81(10):1370–9. • Wilder DG, Aleksiev AR, Magnusson ML, et al: Muscular response to sudden load: A tool to evaluate fatigue and rehabilitation. Spine 1996;21:2628–39