Understanding Cognitive Impairment and Falls in Older People
290 likes | 509 Vues
Explore the impact of cognitive disorders on fall risk in elderly individuals and learn about the Mini-Mental Status Exam for cognitive assessment.

Understanding Cognitive Impairment and Falls in Older People
E N D
Presentation Transcript
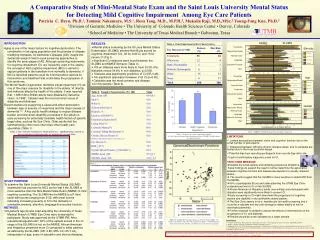
Falls in older people have a major impact on health, healthcare costs and quality of life. The prevalence of falls in elderly people with cognitive disorders is dramatically higher than in older adults without cognitive impairment.
Patients with dementia include those with a diagnosis of Alzheimer's disease, vascular dementia, Lewy-Body dementia, fronto-temporal lobe dementia, and those associated with other disorders. Such patients normally have slower reaction times and demonstrate impaired judgment. In addition, these patients often have impaired mobility, have poor baseline functional status and impaired strength, and are at higher risk for significant polypharmacy, all of which are known to place patients at higher risks for falls. • Cognitive impairment has been well established as a risk factor for falls.
In one study (Tinetti, 1995 [B]), the relative risk of falling for patients with an Mini-Mental Status Exam (MMSE) of less than 20 was 95% Patients with preexisting cognitive dysfunction often have impaired executive functioning and lose insight, particularly with the inability to differentiate between a safe and unsafe environment.
Mini Mental Status Exam • The Mini-Mental Status exam, created by Folstein in 1975, it is a widely used method that allows clinicians to assess clients in a shorter period of time. The purpose of the exam is to address cognitive functioning. It is typically used to screen for dementia and to monitor its progression. It is also useful for screening specific mental disorders such as Alzheimer disease. Today, due to the availability of more effective treatments for these types of conditions, it is being used as a tool for evaluating treatment effect. During the examination, it is important that the examiner does the following: • Ask open questions • Allow the client to explain things in his/her own words, encouraging the client to elaborate and expand • Avoid interruptions • Avoid “why” questions • Listen carefully and observe the client
MMSE[Cognitive Domains] • Orientation/Time 5 points • Orientation/Place 5 points • Registration 3 points • Attention/Calculation 5 points • Recall of Three Words 3 points • Language 8 points • Visual Construction 1 point
It is very important to score each item as objectively as possible and according to the scoring instructions provided. Although it is clinically useful and important to note any physical impairment and/or sensory deficit that may affect the examinee’s ability to correctly respond to the MMSE items, such factors should not influence your judgment when scoring the items. For example, do not score 1 point for writing a sentence because you believe the individual would have been able to do so if he or she had been wearing his or her glasses at the time. An error in any task should be scored as a zero. • The examinee’s total MMSE score is calculated by summing all of the item scores across the 11 categories. The maximum possible total MMSE score is 30 points. • Unless you are a clinician or other trained professional who is qualified to both interpret the MMSE and conduct a full mental status examination, you should refrain from offering any judgments about the examinee’s cognitive state. If he or she asks for the score or the test results, you should not provide the information unless you are qualified and prepared to also provide the appropriate interpretation of the score and a clear and simple explanation of what the results mean.
Mini Mental Status Examination I • The MMSE covers: • Appearance • Behavior and Psychomotor Activity • Attitude Toward Examiner • Speech • Orientation and Consciousness • Mood and Affect • Perceptual • Thinking • Concentration and Attention • Memory • Demonstrated Defenses • Insight into Difficulties
Mini Mental Status Examination • Appearance • Dress (neat, disheveled, unkempt) • Grooming & Hygiene • Behavior and Psychomotor Activity • Gestures • Twitches • Restlessness • Agitation • Stupor • Attitude Toward Examiner • Cooperative • Friendly • Playful • Guarded/Defensive • Suspicious/Hostile • Open/Frank • Speech • Minimal (mostly "yes" and "no" answers, little volunteered information) • Talkative • Rapid/Pressured (as in possible hypomania or mania)
What an MSE isn’t • An intelligence test • A detailed memory test • A fully precise measure of cognition, affect, and behavior
Yet the score is considerably influenced by the culture, language, education and age of the patient, not counting visual and hearing impairment. Depending on the support system, some individuals can function within their home environment at a very low MMSE score. Some years ago, I encountered an elderly couple who continued to live on their own, despite a combined MMSE score of only 12.
Practical ways of managing our increasingly frail and confused patients would be very helpful! • OVER TO YOU!
SYMPTOMS & SIGNS OF AD Memory impairment Gradual onset, progressive cognitive decline Behavior and mood changes Difficulty learning, retaining new information Aphasia, apraxia, disorientation, visuospatial dysfunction Impaired executive function, judgment Delusions, hallucinations, aggression, wandering
NORMAL LAPSES vs DEMENTIAExamples (1 of 2) Forgetting a name Leaving kettle on Finding right word Forgetting date or day Not recognizing family member Forgetting to serve meal just prepared Substituting inappropriate words Getting lost in ownneighborhood
NORMAL LAPSES vs DEMENTIAExamples (2 of 2) Trouble balancing checkbook Losing keys, glasses Getting blues in sad situations Gradual changes with aging Not recognizing numbers Putting iron in freezer Rapid mood swings for no reason Sudden, dramatic personality change
DEPRESSION vs DEMENTIA: The symptoms of depression and dementia often overlap Late life depression can herald impending dementia In general, patients with primary depression: Demonstrate motivation during cognitive testing Express cognitive complaints that exceed measured deficits Maintain language and motor skills
Risk Factors for AD Age Family history Head injury Fewer years of education Down’s Syndrome Metabolic Syndrome? Inactivity? Vascular disease risk factors
MMSE[Influences] • Educational Level • Race / Ethnicity • Socioeconomic Status?