PARKINSONISM
PARKINSONISM. Susie Ro, M.D. Movement Disorders Center Swedish Neuroscience Institute Seattle, WA September 13, 2014. OBJECTIVES. RECOGNIZE CLINICAL FEATURES of PARKINSONISM IDENTIFY “ RED FLAGS ” for ATYPICAL PARKINSONISM BE VIGILANT for SECONDARY PARKINSONISM

PARKINSONISM
E N D
Presentation Transcript
PARKINSONISM Susie Ro, M.D. Movement Disorders Center Swedish Neuroscience Institute Seattle, WA September 13, 2014
OBJECTIVES • RECOGNIZE CLINICAL FEATURES of PARKINSONISM • IDENTIFY “RED FLAGS” for ATYPICAL PARKINSONISM • BE VIGILANT for SECONDARY PARKINSONISM • EARLY DETECTION/ PREVENTION? • ALGORITHMIC APPROACH TO DIAGNOSIS AND TREATMENT of PARKINSONISM
WHAT IS PARKINSONISM? “PARKINSONISM” = Clinical syndrome of stiffness (rigidity), slowness (bradykinesia) +/- tremor Most commonly due to iPD, but may be due to another degenerative process, or secondary to another cause “PARKINSON DISEASE” = specific disorder (idiopathic Parkinson Disease), 2nd most common adult onset movement disorder, affecting >1 million Americans
PARKINSON’S DISEASE Progressive loss of dopamine-producing neurons in the SNPC causes an imbalance in the circuits controlling movement. Motor symptoms are treated by increasing dopamine stimulation
DIAGNOSTIC CRITERIA for iPD (UK BRAIN BANK) STEP 1: BRADYKINESIA + at least 1 of the following: A. RIGIDITY B. 4-6 Hz RESTING TREMOR *1/3 of PD patients have no tremor * PD patients may only have “action tremor” C. POSTURAL INSTABILITY (not caused by primary visual, vestibular, cerebellar, or proprioceptive dysfunction) STEP 2: EXCLUDE OTHER CAUSES of PARKINSONISM STEP 3: AT LEAST 3 OF THE FOLLOWING A. UNILATERAL ONSET *remains asymmetric B. REST TREMOR C. PROGRESSIVE DISORDER D. PERSISTENT ASYMMETRY (first side worse) E. EXCELLENT RESPONSE to L-DOPA (70-100%) F. SEVERE L-DOPA-INDUCED CHOREA *fluctuations not specific G. L-DOPA RESPONSE >5 YEARS H. CLINICAL COURSE of >10 YEARS
PD vs. ESSENTIAL TREMOR (ET) -ET: Often familial (50-70%), slowly progressive (>20 yr Hx unlikely PD) but ET and PD may coexist (shared risk factor?) -often responsive to alcohol, worse with stress/ fatigue, smoking, and sometimes stimulants (but not specific to ET) -Action > distal postural tremor of the arms, but may also affect head, trunk. Leg tremor, marked asymmetry, or rest tremor less common. -Frequency 4-12 Hz, inverse relationship between amplitude and rate which progresses over time, not slowed by mass loading -Head/ vocal tremor may occur in isolation (also tongue/ chin), but isolated head tremor with torticollis likely dystonia Action tremor ≠ “intention tremors” ET is not the only cause of action/ intention tremors PD is not the only cause of resting tremors It is the bradykinesia/ rigidity that defines parkinsonism
DIAGNOSTIC ACCURACY: LOW AAN 2014: ProbPD (L-Dopa responsive) vs. PossPD (never treated or not clearly responsive) AZSAND: (Arizona Study of Aging and Neurodegenerative Disorders, an ongoing longitudinal clinico-neuropathologic study): PD duration <5 years, only 53% had PD at autopsy (8/15). >5 years, often with dyskinesia, 88% (72/82) Overall accuracy 82% (80/97) of ProbPD, 26% (9/34) of PossPD at first visit UK PD Society Brain Research Centre Brain Bank criteria 99% DATATOP: 92% at 7.6 years follow up (not all pathologically confirmed)
DaT SCAN Dopamine Transporter SPECT scan -FDA approved since 2011 to differentiate between ET (essential tremor) and Parkinsonian syndromes -Cannot reliably differentiate between different parkinsonian syndromes (e.g. iPD, MSA, PSP) -Can be useful to differentiate from DIP (drug-induced parkinsonism) and others (?vascular? ?psychogenic?)
MSA MULTIPLE SYSTEM ATROPHY: term first coined by Graham and Oppenheimer (1969) MSA = PARKINSONISM (often more rapidly progressive) + AUTONOMIC/ CEREBELLAR/ PYRAMIDAL SIGNS + SEVERE SPEECH/ SWALLOWING/ BALANCE PROBLEMS EARLY IN COURSE + POOR/ TRANSIENT RESPONSE TO L-DOPA +/- ADDITIONAL FEATURES (e.g. Peripheral neuropathy, Abnormal eye movements) Seen in iPD but rare in MSA: anosmia*, hallucinosis DYSKINESIAS ARE POSSIBLE IN MSA, ESPECIALLY CRANIOCERVICAL
MSA Subtypes 1. MSA-A (Autonomic) Shy and Drager (1960) a.k.a. SHY DRAGER SYNDROME 2. MSA-C (Cerebellar) Dejerineand Thomas (1900) a.k.a. SPORADIC OLIVOPONTOCEREBELLAR ATROPHY (OPCA) DDx: SCA 3, cerebellar degeneration 3. MSA-P (Parkinsonian) a.k.a. STRIATONIGRAL DEGENERATION (SND) Early onset falling Severe dysarthria and dysphonia Respiratory stridor Anterocollis Pyramidal signs
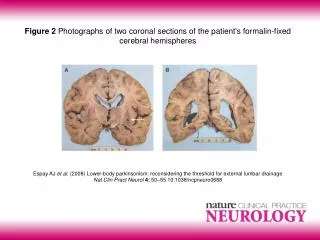
MSA/ PD-PATHOLOGY Papp et al. (1989): Neural and Filamentous a-synuclein containing glial cytoplasmic inclusions (GCIs) Preganglionic (vs. PD which is postganglionic) Can have REMBD but usually not anosmia
MSA-IMAGING T2 signal in putamen, “hot cross bun” sign in pons, Pontocerebellar atrophy, T2 signal in MCP (OPCA), ?Diffusion Tensor Imaging? ?PET/ SPECT?
PSP (Progressive Supranuclear Palsy) Stiff, broad-based gait with slight extension of trunk/ legs armswing can be present, marked axial rigidity, rest tremor rare “Stunned” facial expression; “procerus sign” EOM/ Eyelid abnormalities (wide-eyed/ eyelids closed, can’t look down) Bulbar (dysarthria, dysphagia) and pseudobulbar palsy, Dementia (frontal dysfunction) PSP“Hummingbird Sign” Olfactory sparing No/ poor response to sinemet; motor fluctuations rare
CBS CORTICOBASAL GANGLIONIC SYNDROME (a.k.a. “Parietal Pick’s Disease”) • Markedly ASYMMETRIC Parkinsonism with mainly rigidity/ bradykinesia/ postural instability and DYSTONIA, can have tremor and MYOCLONUS • “Alien Hand” Syndrome (“anterior”/ motor type); spontaneous elevation of limbs • APRAXIA (ideomotor and ideational), the “useless hand”, cortical sensory loss • Frontal/ cortical dementia, language/ speech alterations • Oculomotor findings (may be confused with PSP) • Onset mean age, death by 8 years, M:F 3:2
FRONTOTEMPORAL DEMENTIA/ FTLD (PICK’s DISEASE) “KNIFE-EDGE” GYRI due to marked frontotemporal atrophy • Prominent frontal lobe dementia • Personality changes (disinhibition/ inappropriate behavior, apathy/ euphoria) • Aphasia • Parkinsonian features
SECONDARY PARKINSONISM Infectious/ Postinfectious: Viral, Syphilis, TB, Whipple’s, Prion, fungal, etc. Drug-induced: NEUROLEPTICS, ANTIEMETICS, Monoamine depleters, Amiodarone, VPA, Li+, Ca channel blockers, etc. Metabolic: Acquired hepatocerebral degeneration, cerebrotendinous xanthomatosis, ceroid lipofuscinosis, hemochromatosis, Niemann-Pick Type C, Folate deficiency, BG calcification Toxic: CO, Manganese, MPTP, MeOH, CN, insecticides, etc. Structural: Vascular: multi-infarct, anoxic encephalopathy NPH: (Normal Pressure Hydrocephalus), etc.
NPH (Normal Pressure Hydrocephalus) 3 W’s: “wet, wacky, wobbly” 1. Frontal urinary incontinence • Subcortical dementia • “Magnetic gait”: wide-based, slow/ shuffly, freezing CSF acqueductal flow MRI High-volume LP or lumbar drain NPH is potentially curable…but only if treated early!
SECONDARY PARKINSONISM(IF IT DOESN’T LOOK LIKE iPD, GET AN MRI) Manganese Poisoning T1 Globus Pallidus Carbon Monoxide ( T2 putamen)
“RED FLAGS”SUMMARY Hx of neuroleptic use, toxic exposure, stroke, etc. Supranuclear gaze abnormalities, spastic/ dysarthric speech Prominent autonomic, pyramidal, cerebellar signs or other unexplained signs (neuropathy, amyotrophy) Early or severe falls, dementia, apraxia/ aphasia, pseudobulbar palsy Marked asymmetry/ lack of asymmetry Rapid progression or stepwise clinical course POOR OR TRANSIENT RESPONSE TO LEVODOPA
ALGORITHIM forPARKINSONISM TAKE HOME MESSAGES: -(Nearly) everyone deserves a trial of levodopa -If L-dopa doesn’t work, get an MRI, refer -Do not miss DIP or NPH
Parkinson’s Disease EARLY DETECTION? MEDICAL MANAGEMENT/ AVOIDING PITFALLS SURGICAL MANAGEMENT
PRE-MOTOR PARKINSON’S PD is not just a motor disease…. Non-motor symptoms appear first. By the time the first motor symptoms appear, 70% of dopaminergic activity is gone Braak H et al. Staging of brain pathology related to sporadic Parkinson’s dosease/. Neurobiol Aging 2003;24:197-211. Schapira AH et al. Perspectives on recent advances in the understanding and treatment of Parkinson’s disease. Eur J Neurol. 2009;16:1090-1099.
PRE-MOTOR DETECTION? GENETIC TESTING TISSUE BIOPSY for a-synuclein COLON SALIVARY GLAND BIOMARKERS OLFACTORY TESTING (e.g. UPSIT) OCT VOICE ANALYSIS SCREENING FOR REMBD, DEPRESSION, CONSTIPATION IMAGING DaT and other radioligands DTI (Diffusion Tensor Imaging), 7T MRI? MIBG SPECT (cardiac) Transcranial U/S
PREVENTION? DISEASE MODIFICATION? CAUSE(S) of iPD are still not well understood. -Genetic studies: hints to abnormal protein handling -”prion-like” spread of abnormal protein aggregation (a-synuclein -> Lewy Bodies) NO KNOWN PREVENTION (and by motor stage, the “horse is out of the barn”) PREMOTOR (or PRECLINICAL?) DETECTION + DISEASE MODIFICATION (or halting progression?) vs. “replacement therapy” (i.e. stem cell implantation)
PREVENTION? DISEASE MODIFICATION? a-synuclein VACCINATION? Monoclonal Ab? (block “transmission” of misfolded a-synuclein EARLY MAO-B INHIBITION? EXERCISE/ DIET? CAFFEINE?
PD-MEDICATIONS • DOPAMINERGIC • L-Dopa (Sinemet, Stalevo, Parcopa) • DA Agonists (Pramipexole, Ropinirole, Rotigotine, Apomorphine) • MAO-B inhibitors (Selegiline, Zydis Selegiline, Rasagiline) • COMT inhibitors (Entacapone, Tolcapone) • OTHER • Anticholinergics (Trihexphenidyl, Benztropine, Procyclidine, Profenamine, Orphenadrine) • Amantadine
DA DA Sites of Action of Parkinson’s Disease Drugs Periphery Brain Blood-Brain Barrier Neuron 3-OMD COMT Inhibitors L-DOPA L-DOPA MAO-B Inhibitors AADC DOPAC Carbidopa DA DA DA DA DA 3-MT COMT Inhibitor* Dopamine receptors Dopamine agonists 3-OMD=3-O-methyldopa *Only tolcapone inhibits COMT in brain.
PD MEDS • L-dopa- still the gold standard, most “bang for buck” with fewest side effects, cheapest cost, but short-acting; may lead to motor fluctuations • DA agonists- helps reduce/ delay motor fluctuations but higher side-effect to efficacy ratio compared to levodopa • COMT inhibitors- used only as adjunct to levodopa to reduce motor fluctuations • MAO-B inhibitors- initial or adjunctive therapy ?disease modifying? (see below)
Sinemet(carbidopa/levodopa)- the “Gold Standard” • Dopamine precursor • Administered with carbidopa to prevent peripheral conversion of dopamine • Several formulations- KNOW DOSES and TIMES! • IR 10/100, IR 25/100, IR 25/250, CR 25/100, CR 50/200 • Stalevo 50, 75, 100, 125, 150, 200 • CR (controlled release) vs. IR (regular) • CR is 30% less efficacious, less predictable absorption, does not prolong ON time, but gentler profile Tolosa et al. Neurology. 1998;50 (suppl 6):S2-S10; discussion S44-S48. Olanow et al. Neurology. 2001;56 (suppl 5):S1-S88. Jankovic and Tolosa. Parkinson’s Disease and Movement Disorders. 3rd ed. Philadelphia: Lippincott Williams & Wilkins; 1998:177-190. Sinemet (carbidopa-levodopa). Complete prescribing information. Merck & Co. Inc.; Bristol-Myers Squibb Co.; April 2002. Barbosa et al. Psychiatr Clin North Am. 1997;20:769-790.
DOPAMINE AGONISTS • Older (ergots cause cardiac valve fibrosis) • Bromocriptine and Pergolide no longer used in PD • Newer • Rotigotine (Neupro patch) back on the market • Pramipexole (Mirapex) and Mirapex XR • Ropinirole (Requip) and Requip XL • Apomorphine (Apokyn) injections (nasal spray?) PROS: longer lasting, lessens/ postpones motor fluctuations and need for levodopa CONS: more dopaminergic side effects, weaker than levodopa, more expensive
Common Side Effects of Dopaminergic Drugs (and what to do about them!) • Nausea • slow titration, small amount of non-protein food • avoid reglan, compazine, phenergan; can use lodosyn, tigan, zofran; ?sinemet CR? • Drowsiness – beware “sleep attacks” and driving • slow titration, treat any sleep disorders, use stimulants • Dizziness - often due to low BP (orthostatic hypotension) • lower BP meds, stop/ decrease DA agonists, smaller more frequent doses of sinemet • increase fluid/ salt intake, drink water with sinemet, compression stockings, florinef/ midodrine
Common Side Effects of Dopaminergic Drugs (and what to do about them!) • Confusion/ Hallucinations • Decrease DA agonists, anticholinergics/ amantadine +/- sinemet • Add seroquel or memory drugs (avoid haldol, risperdal, abilify, etc.) • Dyskinesias • Decrease sinemet, smaller more frequent doses • Add adjuncts such as Azilect, Comtan to lessen wearing off, or Amantadine to lessen dyskinesia • Compulsive behavior • Decrease/ stop dopamine agonists • Antidepressants, counseling • Leg swelling • Decrease/ stop dopamine agonists, compression stockings, diuretics
MAO-B INHIBITORS • Slows breakdown of both endogenous and exogenous dopamine • Benign side effect profile (OK with normal diet, SSRIs, etc), but only mild symptomatic benefit • Mainly useful as symptom stabilizer and prolonging duration of levodopa effect (less wearing off) • Available formulations • Selegiline (Eldepryl) • Amphetamine metabolites • Zydis selegiline (Zelapar) • Rasagiline (Azilect)
(n=404) (n=324) (n=272) (n=237) (n=206) (n=164) TEMPO: Mean Change in Total UPDRS at 6-Year Follow-Up * ITT Population (n = 404) 80 * Delayed Start Early treatment * 70 60 * P<0.05 *** P<0.001 50 * Mean % Change in Total UPDRS 40 * 30 * *** 20 10 Years 0 0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 5.5 6.0 Overall difference between Early and Delayed Start Rasagiline groups is 16% (P=0.006) Hauser RA, et al. Mov Disord. 2008;24:562-571.
OTHER PD MEDS • Amantadine- • Flu drug: helps mainly rest tremor and levodopa-induced dyskinesias, • not great in elderly- hallucinations, leg swelling, kidney problems? • Anticholinergics(e.g. trihexphenidyl) • helps mainly rest tremor, slight effect on rigidity, no help to bradykinesia, • high risk of side effects (memory problems, constipation, dry mouth, blurry vision)
Initiation of Drug Tx for PD Adapted from Schapira AHV, Arch Neurol. Aug 2007;64(8): 1083-8
Mild Moderate Severe Disease Severity Dyskinesia, “On-Off” Motor Fluctuations Postural Instability, Freezing, Falls, Dementia Signs of levodopa“wearing-off” Patient Symptoms Agonists, MAOB Inhib Levodopa, COMT inhibitors, others Treatment DBS PD Treatment: Continuum of Interventions Modified from Giroux, ML and Farris, SF. Cleveland Clinic Foundation 2005 Cleveland Clinic Foundation, Center for Neurological Restoration
How does DBS work? Uses an implanted electrode to deliver high-frequency electrical stimulation to structures involved in the control of movement This electrical stimulation helps control motor symptoms by overriding abnormal neuronal activity within these brain regions
Dyskinesia Before After “On” Time “Off” Time This graph is only for illustrative purposes and does not represent actual “on” and “off” time. DBS lessens motor fluctuations
DBS, YES or NO? • Good function on meds, but disabling motor fluctuations (wearing off, failed doses, dyskinesias) or Refractory tremor EFFECTIVE: “BETTER THAN BEST MEDICAL TX” • 5 hours/day more ON time without dyskinesia, 80-90% tremor suppression • Reduce medication doses 20-70%, side effects • Can help some nonmotor symptoms such as sleep, bladder function, weight loss WHAT IT CANNOT DO: • Does NOT slow down/ cure PD, allow patients to quit all meds • Does NOT make patients better than their best ON state • Does NOT help certain symptoms of PD that do not respond to levodopa, such as memory and certain types of balance, speech problems