
Introduction
Familial Isolated Duodenal Atresia (FIDA) A Case Report of Type III Duodenal Atresia. Pratikkumar Patel MD, MPH PGY-2, Angela Flores MD, Maria Teresa Ambat, MD Texas Tech University Health Science Center Paul L.Foster School of Medicine at El Paso. Introduction. Discussion.

Introduction
E N D
Presentation Transcript
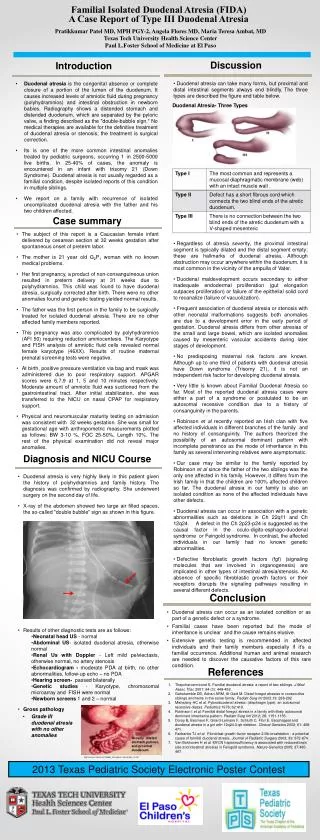
Familial Isolated Duodenal Atresia (FIDA) A Case Report of Type III Duodenal Atresia Pratikkumar Patel MD, MPH PGY-2, Angela Flores MD, Maria Teresa Ambat, MD Texas Tech University Health Science Center Paul L.Foster School of Medicine at El Paso Introduction Discussion • Duodenal atresia can take many forms, but proximal and distal intestinal segments always end blindly.The three types are described the figure and table below. • Regardless of atresia severity, the proximal intestinal segment is typically dilated and the distal segment empty; these are hallmarks of duodenal atresia. Although obstruction may occur anywhere within the duodenum, it is most common in the vicinity of the ampulla of Vater. • Duodenal maldevelopment occurs secondary to either inadequate endodermal proliferation (gut elongation outpaces proliferation) or failure of the epithelial solid cord to recanalize (failure of vacuolization). • Frequent association of duodenal atresia or stenosis with other neonatal malformations suggests both anomalies are due to a development error in the early period of gestation. Duodenal atresia differs from other atresias of the small and large bowel, which are isolated anomalies caused by mesenteric vascular accidents during later stages of development. • No predisposing maternal risk factors are known. Although up to one third of patients with duodenal atresia have Down syndrome (Trisomy 21), it is not an independent risk factor for developing duodenal atresia. • Very little is known about Familial Duodenal Atresia so far. Most of the reported duodenal atresia cases were either a part of a syndrome or postulated to be an autosomal recessive condition due to a history of consanguinity in the parents. • Robinson et al recently reported an Irish clan with five affected individuals in different branches of the family and no history of consanguinity. The authors theorized the possibility of an autosomal dominant pattern with incomplete penetrance as the mode of inheritance in this family as several intervening relatives were asymptomatic. • Our case may be similar to the family reported by Robinson et al since the father of the two siblings was the only one affected in his family. However, itdiffers from the Irish family in that the children are 100% affected children so far. The duodenal atresia in our family is also an isolated condition as none of the affected individuals have other defects. • Duodenal atresia can occur in association with a genetic abnormalities such as deletions in Ch 22q11 and Ch 12q24. A defect in the Ch 2p23-p24 is suggested as the causal factor in the oculo-digito-esphago-duodenal syndrome or Feingold syndrome. In contrast, the affected individuals in our family had no known genetic abnormalities. • Defective fibroblastic growth factors (fgf) (signaling molecules that are involved in organogenesis) are implicated in other types of intestinal atresia/stenosis. An absence of specific fibroblastic growth factors or their receptors disrupts the signaling pathways resulting in several different defects. • Duodenal atresia is the congenital absence or complete closure of a portion of the lumen of the duodenum. It causes increased levels of amniotic fluid during pregnancy (polyhydramnios) and intestinal obstruction in newborn babies. Radiography shows a distended stomach and distended duodenum, which are separated by the pyloric valve, a finding described as the "double-bubble sign.“ No medical therapies are available for the definitive treatment of duodenal atresia or stenosis; the treatment is surgical correction. • Its is one of the more common intestinal anomalies treated by pediatric surgeons, occurring 1 in 2500-5000 live births. In 25-40% of cases, the anomaly is encountered in an infant with trisomy 21 (Down Syndrome). Duodenal atresia is not usually regarded as a familial condition, despite isolated reports of this condition in multiple siblings. • We report on a family with recurrence of isolated uncomplicated duodenal atresia with the father and his two children affected. Duodenal Atresia- Three Types Case summary • The subject of this report is a Caucasian female infant delivered by cesarean section at 32 weeks gestation after spontaneous onset of preterm labor. • The mother is 21 year old G2P1 woman with no known medical problems. • Her first pregnancy, a product of non-consanguineous union resulted in preterm delivery at 31 weeks due to polyhydramnios. This child was found to have duodenal atresia, surgically corrected after birth. There were no other anomalies found and genetic testing yielded normal results. • The father was the first person in the family to be surgically treated for isolated duodenal atresia. There are no other affected family members reported. • This pregnancy was also complicated by polyhydramnios (AFI 50) requiring reduction amniocentesis. The Karyotype and FISH analysis of amniotic fluid cells revealed normal female karyotype (46XX). Results of routine maternal prenatal screening tests were negative. • At birth, positive pressure ventilation via bag and mask was administered due to poor respiratory support. APGAR scores were 6,7,9 at 1, 5 and 10 minutes respectively. Moderate amount of amniotic fluid was suctioned from the gastrointestinal tract. After initial stabilization, she was transferred to the NICU on nasal CPAP for respiratory support. • Physical and neuromuscular maturity testing on admission was consistent with 32 weeks gestation. She was small for gestational age with anthropometric measurements plotted as follows: BW 3-10 %, FOC 25-50%, Length 10%. The rest of the physical examination did not reveal major anomalies. Diagnosis and NICU Course • Duodenal atresia is very highly likely in this patient given the history of polyhydramnios and family history. The diagnosis was confirmed by radiography. She underwent surgery on the second day of life. • X-ray of the abdomen showed two large air filled spaces, the so-called "double bubble" sign as shown in this figure. • Results of other diagnostic tests are as follows: • Neonatal head US - normal • Abdominal US- isolated duodenal atresia, otherwise normal • Renal Us with Doppler - Left mild pelviectasis, otherwise normal, no artery stenosis • Echocardiogram - moderate PDA at birth, no other abnormalities, follow-up echo – no PDA • Hearing screen- passed bilaterally • Genetic studies - Karyotype, chromosomal microarray and FISH were normal • Newborn screens 1 and 2 – normal • Gross pathology Conclusion • Duodenal atresia can occur as an isolated condition or as part of a genetic defect or a syndrome. • Familial cases have been reported but the mode of inheritance is unclear and the cause remains elusive. • Extensive genetic testing is recommended in affected individuals and their family members especially if it’s a familial occurrence. Additional human and animal research are needed to discover the causative factors of this rare condition. References Thepcharoennirund S. Familial duodenal atresia: a report of two siblings. J Med Assoc Thai, 2001; 84 (3): 448-452. Gahukamble DB, Adnan ARM, Al-Gadi M. Distal foregut atresias in consecutive siblings and twins in the same family. Pediatr Surg Int 2003;19: 288-292 Mishalany HC et al. Pyloroduodenal atresia: (diaphragm type): an autosomal recessive diseas. Pediatrics 1978; 62:419. Robinson I et al. Familial distal foregut atresia in a family with likely autosomal dominant inheritance pattern. Pediatri Surg Intl 2012; 28: 1151-1155. Doray B, Becmeur F, Girard-Lemaire F, Schluth C, Flori E. Esophageal and duodenal atresia in a girl with 12q24.3-qtr deletion. Clinical Genetics 2002; 61: 468-471. Fairbanks TJ et al. Fibroblast growth factor receptor 2 IIIb invalidation - a potential cause of familial duodenal atresia. Journal of Pediatric Surgery 2003; 39: 872-874. Van Bokhoven H et al. MYCN haploinsufficiency is associated with reduced brain size and intestinal atresias in Feingold syndrome. Nature Genetics 2005; 37:465-467. • Grade III duodenal atresiawith no other anomalies Grossly dilated stomach,pylorus, and proximal duodenum http://courses.md.huji.ac.il/96854_e/Duodenal_atresia/slide_14.htm 2013 Texas Pediatric Society Electronic Poster Contest





